Chapter 13 Posterior Mini-Incision Hamstring Harvest Approach for Anterior Cruciate Ligament Reconstruction*
Overview
Hamstring (HS) use for anterior cruciate ligament reconstruction (ACLR) has increased greatly in the past 5 years as improved fixation techniques have allowed stability rates to meet or exceed those of bone–patellar tendon–bone (BPTB) grafts.1 It has been said that the harvest is the most difficult part of HS ACLR2 and may require a learning curve of roughly 50 procedures.3
Anatomy
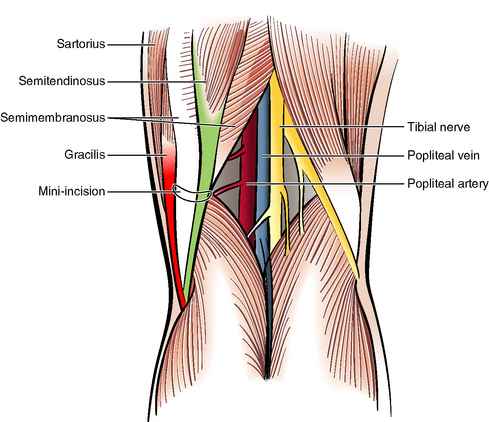
The accessory ST tendon is the primary structure leading to premature amputation of the ST tendon after tendon harvesting. This structure is not described in any standard anatomy texts. However, several papers have described it.4–6 It is present in about 70% of patients. Other cross-connections exist variably from the ST and Gr tendons. In some patients they are thin and will be easily cut with a tendon stripper. However, the accessory ST in particular can be almost as thick as the main trunk of the ST. Especially in these cases, the tendon stripper can easily sever the main trunk of the ST, rendering it too short to use. The variability of the anatomy is such that it is difficult to devise a consistent plan for freeing the tendon using the traditional approach, except to run a scissors along both sides of both tendons. Branches of the saphenous nerve, and indeed its main trunk, are very close by, and saphenous neurapraxia is very common after these dissections. The takeoff of the accessory ST was shown in our studies to be an average of 5 to 6 cm posterior to the tibial crest. Although orthopaedic surgeons rarely operate posteriorly and may be apprehensive about a posterior approach, the posterior approach does not subject neurovascular structures to significant risk. Our cadaver studies showed that the closest neurovascular structure was the popliteal artery, but in eight specimens it was always at least 2.9 cm away from the ST tendon. It was also shielded from the ST tendon by the semimembranosus muscle.
Surgical Technique
Making the Posterior Skin Incision
The ST is the most prominent tendinous structure in the popliteal fossa and runs just medially to the midline. The affected lower extremity is externally rotated, and the knee is flexed about 30 degrees. The surgeon bends over the leg to see posteromedially. The incision should be made directly over it in the popliteal fossa, shading slightly anteromedially (Fig. 13-1). If the ST cannot be felt, the incision can be put into the soft spot in the skin just medial to the midline. The location of this incision is not critical because the tendon can always be found by moving the highly mobile skin in this area. The incision should be made 3 cm in length initially but need only be 2 cm in length once experience is gained. It should be put within or parallel to a skin crease. After the dermis is incised with a #15 blade, the subcutaneous tissue is opened by spreading with Metzenbaum scissors.
Finding the Semitendinosus
An index finger should probe the incision, fishing the tendon out bluntly. If it is not easily found in this manner, two Senne retractors can be used to open the incision, and the tendon can be found under direct visualization. Once the tendon is identified, a right-angle clamp is passed around it. A ¼-inch Penrose drain then captures it and is loosely clamped (Fig. 13-2).

Identifying the Semitendinosus in the Anterior Incision
Related posts:
 The Central Quadriceps Free Tendon for Anterior Cruciate Ligament Reconstruction
The Central Quadriceps Free Tendon for Anterior Cruciate Ligament Reconstruction
 Proprioception and Anterior Cruciate Ligament Reconstruction
Proprioception and Anterior Cruciate Ligament Reconstruction
 Anterior Cruciate Ligament Reconstruction Utilizing the Rigidfix for Femoral-Sided Fixation
Anterior Cruciate Ligament Reconstruction Utilizing the Rigidfix for Femoral-Sided Fixation
 Revision Anterior Cruciate Ligament Reconstruction Using Autologous Hamstring Tendons
Revision Anterior Cruciate Ligament Reconstruction Using Autologous Hamstring Tendons
 High-Stiffness, Slippage-Resistant Cortical Fixation Has Many Advantages over Intratunnel Fixation
High-Stiffness, Slippage-Resistant Cortical Fixation Has Many Advantages over Intratunnel Fixation
 Endobutton Anterior Cruciate Ligament Reconstruction Femoral Fixation
Endobutton Anterior Cruciate Ligament Reconstruction Femoral Fixation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


