Postauricular Flap for Ear Reconstruction
Matthew M. Hanasono
DEFINITION
Reconstruction of auricular defects arising from trauma or oncologic resection aims to restore the natural anatomic structures and landmarks of the ear and ideally should maintain balance and symmetry with the contralateral ear.
Postauricular flaps are useful for reconstructing larger marginal defects of the upper and middle thirds of the auricle and are typically used in combination with cartilage grafts for reconstructing those defects that are too large for wedge or Antia-Buch chondrocutaneous advancement techniques.1
The postauricular flap is also known as the retroauricular flap or the Dieffenbach flap.
Inferiorly based postauricular flaps can also be used for ear lobe reconstruction.
ANATOMY
The outer rim or helix creates the outer curvature of the ear and originates from the face at the root of the helix.
Concentrically, within the helix is the antihelix, which separates into two separate crura in the upper third of the ear that define the triangular fossa.
The scapha is the concave rim that separates the helix and antihelix.
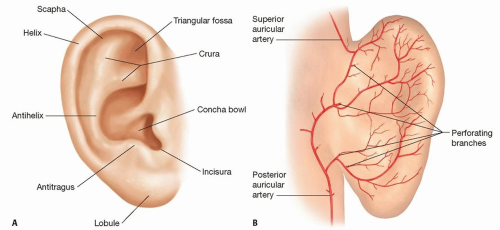
FIG 1 • A. Anatomy of the external ear. B. Arterial anatomy of the posterior ear. (The right ear is shown.) The posterior auricular artery provides the blood supply for the postauricular flap. It anastomoses with the superficial temporal artery via the superior auricular artery.
The concha lies within the antihelix and is the structure that leads to the external auditory meatus.
The anterior border of the external auditory meatus is defined by the tragus.
In the lower third of the ear lies the lobule or ear lobe, which does not contain cartilage (FIG 1A).
The blood supply to the auricle is through the posterior auricular artery and superficial temporal artery.
The posterior auricular artery runs in the sulcus between the auricular cartilage and the mastoid process of the temporal bone.
This vessel supplies the posterior ear skin and posterior auricular muscle and sends perforating branches that pierce the auricular cartilage in the region of the triangular fossa, cymba conchae, cavum conchae, helical root, and ear lobe to supply the anterior ear skin (FIG 1B).2,3
The posterior auricular artery anastomoses with the superficial temporal artery through the superior auricular artery.
Venous drainage is via the posterior auricular vein into the external jugular system and the superficial temporal and retromandibular veins.
This rich anastomotic network of blood vessels is the basis for the postauricular flap.
PATIENT HISTORY AND PHYSICAL FINDINGS
A thorough history and physical should be obtained prior to any operation by paying close attention to significant comorbidities, including smoking history, prior surgeries including scars in the postauricular area, and medications that may predispose the patient to bleeding.
Patients who wear glasses should also be educated in postoperative care and management of incisions.
They may need to remove the earpiece of the glasses on the reconstructed side until adequate healing has occurred, and then replace the earpiece.
Defects resulting from oncologic resection should consider documentation for clear margins or Mohs excision prior to definitive reconstruction.
IMAGING
Patients who have undergone resection for aggressive cutaneous malignancies may require imaging studies or staging and to rule out metastatic disease.
SURGICAL MANAGEMENT
Postauricular flaps used in ear reconstruction can be based in the superior, middle, or inferior postauricular and mastoid region.2
They are indicated for marginal reconstruction, in combination with cartilage grafts to support and give definition to the helix, in a staged manner as originally proposed by Dieffenbach (FIG 2).
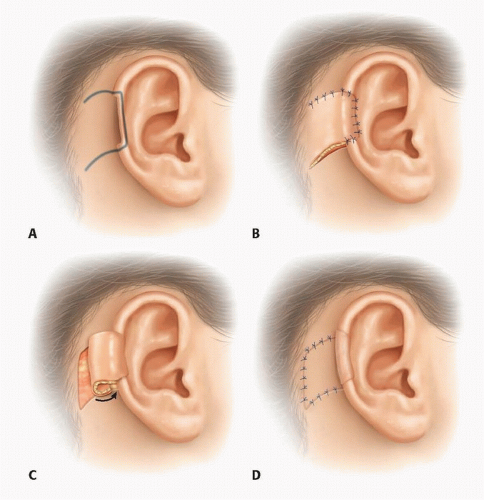 FIG 2 • Method of reconstructing marginal ear defects with the postauricular flap, as originally described by Dieffenbach. The postauricular flap is initially elevated (A), and the flap is transposed from the posterior auricle to the anterior auricle during inset (B). A helical cartilage graft is strongly recommended to preserve the shape of the ear and give definition to the helix, although not included in the original description by Dieffenbach. At a second stage, the base of the flap is divided (C), and the flap donor site is skin grafted (D).
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|