Key Points
Platelet-rich plasma (PRP) for androgenetic alopecia (AGA)
Meta-analyses and systematic reviews suggest PRP can improve hair density in AGA patients.
PRP for alopecia areata (AA)
PRP is a potential option for AA patients. Randomized clinical trials found PRP superior to intralesional triamcinolone acetonide and to minoxidil, but the literature is scant and needs to be replicated.
PRP for cicatricial alopecia (CA)
No randomized, large-scale PRP studies have been conducted in scarring alopecia patients. Only cases series exist to date, thus the success of PRP to treat CA has not been fully investigated.
PRP with surgical hair restoration
PRP can be advantageous in surgical hair restoration procedures as activated platelets can promote tissue repair, minimize scarring, and encourage hair growth.
4.1 Introduction
Platelet-rich plasma (PRP) therapy is a promising nonsurgical option for patients suffering from certain types of alopecia. PRP can provide an alternative option for hair loss patients who are not ideal candidates for traditional treatments and can help avoid commonly reported side effects of other available therapies (e.g., skin irritation and sexual dysfunction). 1, 2, 3, 4, 5, 6 The majority of current evidence explores PRP for management of androgenetic alopecia (AGA) with less data suggesting its use in alopecia areata (AA) and some cicatricial alopecia (CA).
PRP therapy can encourage hair growth through the activity of secreted growth factors and cytokines such as platelet-derived growth factor (PDGF), epidermal growth factor (EGF), and vascular endothelial growth factor (VEGF). 7, 8, 9 Growth factors encourage hair follicles to enter into the then prolong the anagen phase by promoting cell survival, cell proliferation, and angiogenesis through the protein kinase B pathway, inhibition of glycogen synthase kinase 3-β and the degradation of β-catenin ( ▶ Fig. 4.1). 7, 10 PRP can also help decrease inflammation, prevent follicles from prematurely entering the catagen phase, activate proinflammatory signaling pathways, and impact muscle and fat cells. 11, 12, 13, 14
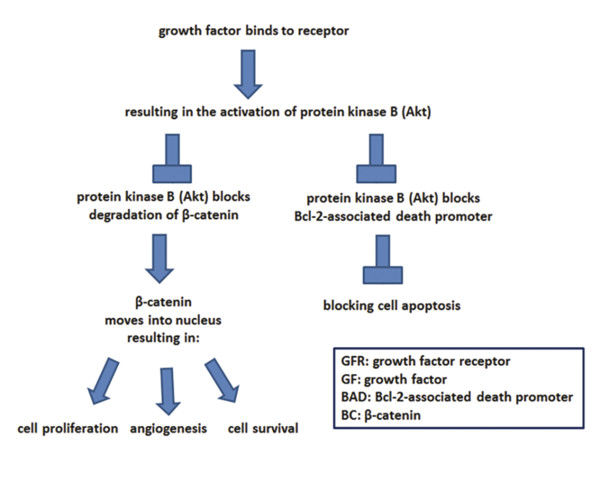
Fig. 4.1 The impact of growth factors on dermal papilla cells. (Adapted from Gupta AK Carviel J. A Mechanistic Model of Platelet-Rich Plasma Treatment for Androgenetic Alopecia. Dermatol Surg Off Publ Am Soc Dermatol Surg Al. 2016;42(12):1335–1339 and Li ZJ, Choi H-I, Choi D-K, Sohn K-C, Im M, Seo Y-J, et al. Autologous platelet-rich plasma: a potential therapeutic tool for promoting hair growth. Dermatol Surg Off Publ Am Soc Dermatol Surg Al. 2012 Jul;38(7 Pt 1):1040–6.)
4.2 PRP for Androgenetic Alopecia
Androgenetic alopecia (AGA) is the most common type of hair loss, characterized by a hair follicles miniaturization, possibly due to increased levels of dihydrotestosterone (DHT) and/or alterations in the androgen receptor gene. 15, 16, 17 These progressive follicular changes lead to a decreased number of hairs in the anagen phase, such that terminal follicles convert into vellus-like follicles. 18 PRP can enhance the limited action of growth factors created by increased DHT levels commonly associated with AGA. 7 The anti-inflammatory effects of PRP could also be advantageous as dermal inflammatory infiltrates and follicular inflammation have been associated with AGA patients. 19, 20, 21
There is great variation in the PRP preparation and application methods used to treat AGA patients. 22, 23, 24, 25, 26 This fact may account for some of the variability in response seen in published observational and randomized clinical trials. A recent meta-analysis reported that PRP was successful in treating patients with AGA, using hair density as the measure of treatment success, as compared to baseline measurements across direct injection studies with an overall standardized mean difference of 0.51 (95% confidence interval: 0.14, 0.88, I2 = 0%, 4 studies). 26 Additionally, in uncontrolled studies, improvements in hair count, hair density, hair thickness, and microscopic evaluations are frequently reported in AGA patients treated with PRP. 22, 24, 25, 27, 28, 29, 30 Erythema, edema, headaches, drowsiness, mild pain, temporary swelling, and scalp sensitivity were among the common side effects reported. 26 The majority of PRP studies conducted in AGA patients are short term, with only a few studies evaluating past 6 months, thus long-term benefits are hard to determine. 24, 25, 30
The highest level of evidence among PRP AGA studies has been provided by Lee et al, who conducted a randomized clinical trial comparing CD34+ cell-containing, leukocyte-rich PRP (PRP + PDRN) to polydeoxyribonucleotide (PDRN) in female pattern hair loss patients (n = 40). 31 PDRN was used in comparison as it can enhance angiogenesis, stimulate wound healing and promote cell regeneration. 32 Twenty patients were treated with 12 weekly sessions of intra-perifollicular PDRN injections, while 20 patients in the active treatment group received 1 session of PRP, followed by 12 weekly sessions of intra-perifollicular PDRN injections. Greater improvement in hair thickness occurred in the PRP + PDRN treatment group as compared to the PDRN comparator (p = 0.031). 31 One week after their final session, improvements in hair counts and hair thickness were noted in both treatment groups as compared to baseline measurements. 31 Evidence of PRP’s success has also been found in recent clinical trials conducted in AGA patients, supporting the use of PRP as a treatment for AGA. 33, 34, 35
4.3 PRP for Alopecia Areata
Alopecia areata (AA, also referred to as spot or patch baldness) is an autoimmune hair loss condition where the immune system attacks actively growing hair follicles. 36 This condition commonly occurs on the scalp but may involve other facial or body hairs and affects both men and women. 37, 38 There are currently no FDA approved therapies for AA; however, many off-label medications (e.g., intralesional triamcinolone, minoxidil) have shown some efficacy. The anti-inflammatory effects of PRP may be of value to these patients. Importantly, studies regarding the management of AA should be interpreted cautiously, since the disease has an unpredictable natural history with spontaneous remissions and relapses.
Intralesional triamcinolone acetonide injections are first-line treatment in many cases of AA. However, a single placebo- and active-controlled, double-blinded, split-scalp, randomized clinical trial found that PRP may be a more efficacious treatment option. Trink et al injected half the scalp in 45 patients with PRP, triamcinolone acetonide, or placebo monthly for 3 months and found a higher success rate, defined as complete remission, among PRP treated lesions (60%) as compared to the steroid (27%). 39 PRP also provided greater success in regrowing fully pigmented hair, with 96% of PRP-treated AA patients regrowing pigmented hairs as compared to 25% of triamcinolone acetonide-treated AA patients. 39 Regrowth in PRP-treated patients has also been reported to occur earlier than minoxidil-treated patients as determined in a placebo-controlled study. 40 This earlier response may not occur in all AA types as PRP is not effective against alopecia totalis. 40 Case reports also suggest that PRP can be a promising treatment for AA. 41
Taken together, there is some evidence that PRP may be beneficial in treating AA. However, studies are few, some lack control, and generally are small in size. The authors have had limited success treating AA with PRP and believe that alternative therapies such as JAK kinases inhibitors are more.
4.4 PRP for Cicatricial Alopecia
Cicatricial alopecia (scarring alopecia) is a rarer class of hair loss comprised of several different and often overlapping conditions such as central centrifugal cicatrical alopecia (CCCA), lichen planopilaris (LPP), frontal fibrosing alopecia (FFA), traction alopecia, etc. All of these diseases result in folliscular damage and eventually permanent replacement with fibrous tissue. 42 Histopathological diagnosis and management of scarring alopecia can be challenging with the primary goal of minimizing inflammation and preserving existing hairs. Restoration options, such as hair transplantation and tissue expansion techniques, can be limited and are only considered after scarring has become fixed. 43, 44, 45 Theoretically, PRP may be of value in these hair loss patients, as it has both regenerative and anti-inflammatory properties.
Evidence supporting the use of PRP in scarring alopecia is limited. There are no large-scale randomized controlled trials, but case studies suggest that PRP may be beneficial in some types of CA. 43 Several months after the combination of a hair transplantation and PRP treatment, an LPP patient was able to achieve a high graft survival rate (approximately 80%), suggesting PRP may be advantageous following surgical hair restoration procedures. 43
While PRP could be beneficial, in the authors’ experience, success is limited for both AA and CA. They believe the future lies in treatment of both conditions with JAK kinase inhibitors (orally and topically) rather than PRP.
4.5 PRP with Surgical Hair Restoration
Follicular unit transplantation (FUT) and follicular unit extraction (FUE) are the main hair transplant options available to AGA patients. During FUT, hair follicles are obtained through the surgical removal of a hair-bearing strip from the back of the scalp. As an alternative to FUT, follicular units can be harvested individually from the donor region using the FUE harvesting technique. During both FUE and FUT, hair follicles are subject to injury or dehydration 46 and thus, less viable. Graft storage solutions containing activated platelets could help with graft preservation and encourage grafts to enter the anagen (growth) phase prior to implantation ( ▶ Fig. 4.2). 10, 47 When grafts were soaked in PRP solution prior to FUT, a 15% increase in hair growth and hair density was reported as compared to grafts soaked in saline solution. 47 PRP can also be used successfully in FUE procedures as evident in a single-blind, randomized study of 40 patients with AGA. 48 In this study, a greater number of PRP treated patients had increased hair regrowth and hair density after FUE as compared to non-PRP treated patients (20/20 = 100% vs. 4/20 = 20% and 12/20 = 60% vs. 0/20 = 0%, respectively). 48
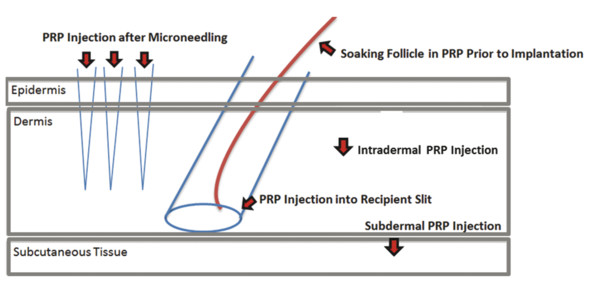
Fig. 4.2 Possible locations to inject PRP. (Adapted from Puig CJ, Reese R, Peters M. Double-Blind, Placebo-Controlled Pilot Study on the Use of Platelet-Rich Plasma in Women With Female Androgenetic Alopecia. Dermatol Surg Off Publ Am Soc Dermatol Surg Al. 2016 Nov;42(11):1243–7, Garg S. Outcome of Intra-operative Injected Platelet-rich Plasma Therapy During Follicular Unit Extraction Hair Transplant: A Prospective Randomised Study in Forty Patients. J Cutan Aesthetic Surg. 2016 Sep;9(3):157–64, and Rogers N. Review of the Literature: Microneedling for Hair Loss? Hair Transpl Forum Int. 2016;26(1):39.)
4.5.1 Important Techniques to Consider
There are a number of important techniques that may be of value when creating a PRP protocol, such as exogenous versus autoactivation. Additional of thrombin and calcium chloride to the solution can activate platelets and trigger degranulation of α-granules. 7, 49, 50 This degranulation can enhance the release of specific growth factors such as insulin-like growth factor 1 (IGF-1) and PDGF. 7, 49, 50 However, activation may not always lead to better hair restoration results. 35 Additionally, activation may not necessarily result in better hair restoration outcomes as significant change in the concentration of some growth factors does not always occur. 24, 25, 27, 28, 35 Thus, further research into identifying which activated growth factors and collection systems can achieve the best hair restoration outcomes is needed. Head-to-head clinical trials will help optimize treatment protocols and inform clinicians about how to best prepare their PRP solutions.
Extracellular matrix (ECM) materials can also be added to PRP to enhance hair restoration outcomes. ECM materials can encourage stem cells to form progenitor cells that may protect dermal papilla cells against the effects of increased DHT levels (e.g., follicle miniaturization). 51, 52 Similar to PRP, ECM materials contain growth factors promoting hair growth such as VEGF, epidermal growth factor (EGF), and insulin like growth factor (IGF). 53, 54 Some regulatory bodies (e.g., FDA) have approved the use of porcine derived urinary bladder ECM material (ACell MatriStem, ACell Inc., Columbia, MD) to help repair and remodel damaged tissues. 55, 56 ECM materials in combination with PRP can be used to improve wound healing and donor scarring during surgical hair restoration procedures. 57, 58, 59 But, products such as Acell contain foreign proteins, so the possibility of a reaction to this material increases the potential for side effects over PRP alone. Furthermore, the increased extracellular pressure of injecting a dense material near follicles could possibly cause negative responses. Without good studies to document improvement with ECM materials and to quantify these risks, it is difficult to substantiate its use. Further research with randomized controlled clinical trials is required as few studies have explored these combined regenerative therapies in alopecia patients.
Single- and double-spin methods can be used to create PRP solutions. 25, 60 The first spin can allow the red blood cells to separate from the plasma. 60 Avoiding high speeds and long durations are encouraged as platelets can be precipitated. 60 Additionally, high concentrations of red or white blood cells in PRP solutions can cause inflammation adjacent to the follicle and be deleterious to hair growth; thus, it is best to limit the amount of red and white blood cells in the final injected preparation. 61 Platelets can be further separated in a second spin. During this second spin, the goal is to precipitate platelets; therefore, higher speeds and longer durations may be helpful. Caution is still advised, however, as high speeds may discharge PDGF from platelets and limit its eventual deposition in the scalp. 60 Both single- and double-spin methods can achieve high volume PRP yields and create desired hair restoration results. 33, 48, 62 Fully automated collection systems, such as the Magellan Autologous Platelet Separator system, can also be used to separate and concentrate platelets. 63
To achieve optimum results, it is suggested that PRP should be performed once a month for 3 months with a platelet concentration of 4 to 7 times a patient’s baseline whole blood levels ( ▶ Fig. 4.3, ▶ Fig. 4.4, ▶ Fig. 4.5, ▶ Fig. 4.6, ▶ Fig. 4.7, ▶ Fig. 4.8, ▶ Fig. 4.9, ▶ Fig. 4.10, ▶ Fig. 4.11, ▶ Fig. 4.12). 64, 65 PRP injections can be administered intradermally, subdermally, and/or placed into premade recipient slits and microneedling channels ( ▶ Fig. 4.2). 34, 48, 66 It is the authors’ opinion that subdermal injections (e.g., Rapaport Subdermal Depo PRP injection) are preferred over intradermal injections, so direct delivery of PRP to the base of the hair follicle can occur. Subdermal injections can also allow for better diffusion of PRP in the loose connective tissue space, effectively coating the hair follicle and decreasing the number of injections necessary to bathe a given area. 67 This technique is well tolerated and may be less painful because as the solution diffuses there is less local pressure than when it exerts pressure on the dermis. These recommendations are only guidelines as standardized PRP procedures have yet to be determined and no studies directly compare one injection technique to the other.

Fig. 4.3 Before and after 9 PRP treatments in a 29-year-old male.
Related posts:
 Platelet-Rich Plasma and Fibrin Sealants in Plastic Surgery: Clinical Applications and One Practice’s Experience
Platelet-Rich Plasma and Fibrin Sealants in Plastic Surgery: Clinical Applications and One Practice’s Experience
 Complications Associated with PRP and Microneedling in Aesthetic Medicine
Complications Associated with PRP and Microneedling in Aesthetic Medicine
 Microneedling: Mechanism and Practical Considerations
Microneedling: Mechanism and Practical Considerations
 Platelet-Rich Plasma for Rejuvenation and Augmentation
Platelet-Rich Plasma for Rejuvenation and Augmentation
 Microneedling: Clinical Applications
Microneedling: Clinical Applications
 Applications and Safety in Skin of Color
Applications and Safety in Skin of Color
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


