26 Planning in Female Hair Transplant Surgery
Summary
Keywords: female-pattern hair loss lichen planopilaris frontal fibrosing alopecia female hairline follicular families double follicular units illusion of density post-op telogen effluvium
Key Points
•Hair loss has a particularly devastating effect in women.
•In evaluating for hair loss in female patients, a thorough personal and family history must be investigated and other medical conditions (lichen planopilaris [LPP], frontal fibrosing alopecia [FFA], polycystic ovarian syndrome (PCOS), etc.) must be excluded before considering a hair transplant surgery.
•Alternative treatments (medical, scalp micropigmentation, hairpiece) should be recommended for female patients who are not surgical candidates.
•Given the diffuse nature of female-pattern hair loss (FPHL), it is difficult to treat all the areas of hair loss. The doctor and the patient should agree as to which area will have the most cosmetic impact after surgery.
•Patient education as to the nature and course of their FPHL is of outmost importance when evaluating patients for their hair loss.
•The use of denser grafts (follicular family [FF] and double follicular unit [DFU]) provides good density if properly positioned in the right areas of the scalp.
•Properly and artistically positioned grafts create the “illusion of density” that will create volume despite the normally limited amount of grafts in female patients.
•All female patients should be educated on the possible post-op sequelae (telogen effluvium, paresthesia, and post-op edema) that may arise after the surgery.
26.1 Introduction
The surgical correction of hair loss in women is perhaps one of the most satisfying aspects of the author’s practice.1 None of our patients are unaffected by their hair loss, or they would not be in our offices. However, the loss is particularly devastating for women. Men with alopecia can make the choice to simply buzz cut their hair and accept their situation; our society does not present that as an acceptable choice for women.
There are other chapters dedicated to nonsurgical therapies used to treat female hair loss. This chapter will focus on surgical treatment, but it is always recommended that patients use adjunctive therapies, in parallel, to help slow the progression of the hair loss. This is very important as a component of the overall long-term planning in women.
Medical Treatment
It is especially important to counsel patients regarding ongoing medical treatment to slow the future loss. This may include hormonal therapies, minoxidil, or platelet-rich plasma (PRP).
26.2 Initial Consultation
Every consultation will include the evaluation of family and medical history and may reveal alopecias that are not amenable to surgery.2,3,4 These topics are covered in Chapters 7, 8, 9 of this textbook as well as many journal articles.5 Women with female-pattern hair loss (FPHL) who are not candidates for hair transplantation most commonly include those who have unrealistic expectations as to what can be achieved with surgery and want a full head of thick hair and women who have diffuse thinning that affects even the potential donor area. These women need to be counseled to seek alternative treatments including medical treatments,6 ,7,,,8 scalp micropigmentation,4 temporary scalp-coloring agents, improved hairstyling, or hairpieces. Other chapters address underlying medical conditions, which can result in alopecia and which should not be treated with surgery, but it is important to be certain that, if indicated, a complete medical assessment, sometimes including a scalp biopsy, has been completed. The increase in incidence of lichen planopilaris (LPP) and frontal fibrosing alopecia (FAA) makes this even more important.9,10
Consultation
The consultation should include a full evaluation of the history of hair loss, including the timeline of potentially related events, and evaluation of the hormonal and nutritional factors that may impact hair loss, as well as a dermoscopic examination. A biopsy, where indicated, should be performed prior to performing surgery.
It is not sufficient in women to cover an area lightly with grafts, as is the approach sometimes in men with limited donor hair. Women already have hair in the area; they are not completely alopecic—the problem is that the hair is perceptively thinner in that area. Depending on the degree of hair loss, this can be very challenging.11,12 To make a true cosmetic impact, density has to be significantly improved and this is done by concentrating the grafts in a smaller area and creating a greater illusion of density with artfully placed grafts (Video 26.1).
Illusion of Density
The artistry in female hair transplantation is extremely important, as the surgeon needs to maximize the illusion of density. This is especially difficult in women, who are not alopecic but have thin hair—to make it look more dense, the grafts need to be concentrated in areas of greatest cosmetic impact.
The choice of which region of the recipient should be treated is a very important part of determining the surgical plan in women. The author usually asks an open-ended question: “If you could thicken one area on your head, show me what that area would be.” If the woman shows me her entire caudal region, it raises a red flag. It is possible that these women will be unhappy with what can be achieved surgically. However, once the limitations of surgery are clearly defined, there are those who will quite quickly reassess their situation and specify a more limited area. It is very important to be certain that female patients considering surgery understand that we cannot address all their areas of concern—only the most important (Fig. 26.1 and Fig. 26.2). There are also hair restoration surgeons (HRS) who mistakenly treat a larger area more lightly to improve density more diffusely. These surgeons usually state that “female patients are difficult to please.”13 This could not be further from the truth!
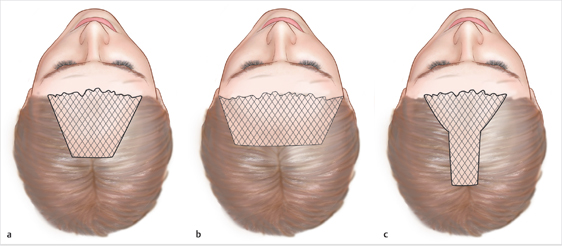
Fig. 26.1 Illustration of planning female hair transplant surgery to maximize cosmetic benefit. The patterns shown are those most commonly utilized by the author to create the most impact from a single surgery. Although many women have enough donor hair for two or three surgeries over their lifetimes, the first surgery should always be performed in the region that will remain the most cosmetically important for the patient. For example, the vertex area may be somewhat problematic for many women; however, with further development of female-pattern hair loss, it will most definitely not be the region of greatest importance. (a) Central frontal region including a deeper portion in a wedge shape that captures some of the part line. This does not generally include the temple recessions but may be made somewhat less deep centrally and include light coverage in the temple regions. (b) Frontal hairline and temple recessions. This is the pattern chosen by women who intend to wear their hair in a style swept backward. The hairline is still always created with a lower density and the transplant increases density ~1 cm posterior. (c) Short frontal zone and part line running further posteriorly toward the midscalp. This is probably the most common pattern chosen. The part line may be central or off to one side. It gives the patient a little more styling flexibility and still addresses the areas that create the facial frame and are noticed most by other people. There is also a variation on this pattern that includes a narrower frontal block region and narrower, longer part line region.
Related posts:
 Methods and Techniques to Study Hair Cell Survival
Methods and Techniques to Study Hair Cell Survival
 Hair Transplantation: The Promise of Cell Therapy
Hair Transplantation: The Promise of Cell Therapy
 The Patient with Minimal Hair Loss: Planning and Decision-Making
The Patient with Minimal Hair Loss: Planning and Decision-Making
 The Young Patient: Planning and Decision-Making
The Young Patient: Planning and Decision-Making
 Hair Anatomy and Histology for the Hair Transplant Surgeon
Hair Anatomy and Histology for the Hair Transplant Surgeon
 East,West, and Southern Asian Hair Transplant Specifics
East,West, and Southern Asian Hair Transplant Specifics
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


