Kloos WE, Torrabene TG, Schleifer KH. Int J Syst Bacteriol 1974; 24: 79–101.
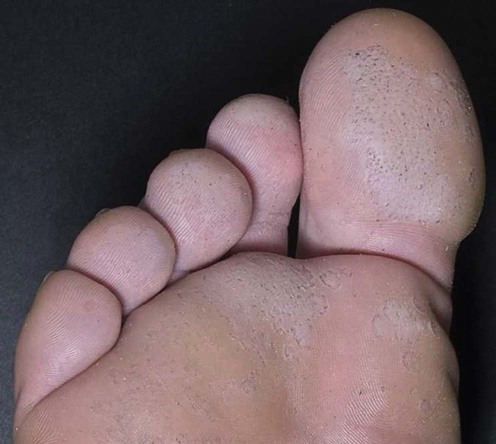
Pitted and ringed keratolysis (keratolysis plantare sulcatum)
Specific investigations
 Wood’s light examination may reveal a coral red fluorescence, but this is not consistently helpful
Wood’s light examination may reveal a coral red fluorescence, but this is not consistently helpful
 Dermoscopy may reveal small black pits in a parallel pattern on the ridges of the stratum corneum
Dermoscopy may reveal small black pits in a parallel pattern on the ridges of the stratum corneum
 Starch iodine test may identify areas of hyperhidrosis
Starch iodine test may identify areas of hyperhidrosis
 Swabs may be obtained for cultures of the organisms
Swabs may be obtained for cultures of the organisms
Isolation and characterization of micrococci from human skin, including two new species: Micrococcus lylae and Micrococcus kristinae.
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree



