div class=”ChapterContextInformation”>
24. Solitary Pigmented Skin Lesion with Surrounding Loss of Pigmentation
Keywords
Halo nevusSuttonLeukoderma acquisitum centrifugum- 1.
Mayerson’s nevus
- 2.
Cockade nevus
- 3.
Halo nevus
- 4.
Regressing melanoma

Solitary pigmented papule on neck surrounded by depigmented skin
Diagnosis
Halo nevus
Discussion
Halo nevus , synonymously known as Sutton’s nevus, perinevoid vitiligo, and leukoderma acquisitum centrifugum, is a melanocytic nevus surrounded by a rim of hypopigmentation or depigmentation [1]. It tends to be multiple in number and usually affects individuals in second decade of life with no gender or racial predilection. The commonest site is upper back followed by neck and abdomen. The central nevus may partially or completely regress in years with or without repigmentation of halo [2].
The development of halo is thought to result from host’s immunologic reactions, chiefly consisting of inflammatory cytokines and cytotoxic CD8+ T cells [3]. The finding of elevated circulating antibodies against melanocytic antigens is only secondary to the destruction of melanocytes.
The typical halo nevus presents as solitary or multiple, darkly pigmented, benign compound melanocytic nevus with a surrounding symmetric, well-defined, rim of depigmented zone. The central papule as well as peripheral halo, both have regular borders. In white skin, it is more appreciable during the summer months showing the non-tanned halo in sharp contrast to the normal skin. The diameter of the halo is correlated to the size of the central nevus, the larger the nevus, the larger the halo. Halo nevi are also associated with vitiligo and a vitiligo-like phenomenon. Approximately 20% of individuals with halo nevi have vitiligo.
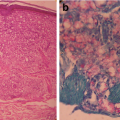
Histopathologically, the nevus may be junctional, compound or dermal, with dense lymphocytic infiltrates surrounding or permeating the dermal component. The nevus cells may become vacuolated with pyknotic nuclei [4]. The use of DOPA stains usually reveal a loss of epidermal melanocytes in the halo area. The peripheral white halo has little or no lymphocytic infiltrate. Regression of the central nevus is not associated with fibrosis, in contrast to the regression of melanoma, due to increased levels of antifibrotic tumor necrosis factor (TNF)-α.
Mayerson’s nevus, cockade nevus and regressing melanoma are usually included in close differential diagnosis of halo nevus.
Mayerson’s nevus : It is clinically presented by a melanocytic nevus developing surrounding eczematous inflammatory reaction associated with epidermal scaling and pruritus. It is usually solitary, but can be multiple and nearly three times as common in males compared to females. The trunk is the most common site, although any site can be affected. Unlike in halo nevus, Meyerson’s nevus does not regress. The histopathology is usually that of an acquired melanocytic nevus with associated spongiotic dermal dermatitis predominated by CD4+ T-lymphocytes that miss other markers of T helper cells such as BCL-6 or CD10 [5].
Cockade nevus : It is a rare variant of acquired melanocytic nevus that peculiarly presents as a target-like nevi, resembling a rosette [6]. There is a hypochromic zone between pigmented central junctional melanocytic nevus and pigmented halo, giving it a target-like configuration. These are usually multiple in number and affect young people. Spinal dysraphism and juvenile diabetes mellitus are its known associations. On histopathology, it does not show cellular infiltrates unlike in halo nevus.
Melanoma : Being an immunogenic tumor and infiltrated by high levels of T lymphocytes, the course of melanoma may witness spontaneous regression with pigmentary changes. It may be clinically evident as depigmentation either within a melanocytic lesion, around melanocytic nevi (halo nevi) or in a distant site (melanoma-associated depigmentation) [7]. Of these, ‘melanoma with a depigmented halo’ simulate the picture of benign halo nevus. Of note, the halo of melanoma is more irregular than that seen in halo nevus and the patients are usually older. To add, histopathology of melanoma with halo during regression reveals fibrous stroma replacing the dermal portion of the tumor [8].
Excisional biopsy is the best recommendation to rule out the possibility of malignancy. However, it can be left keeping under observation.
Key Points
Halo nevus presents as darkly pigmented melanocytic nevus with a surrounding well-defined rim of depigmented skin.
The central nevus may partially or completely regress in years with or without repigmentation of halo.
Regression of the central nevus is not associated with fibrosis unlike in melanoma.
Related posts:
 Years Old Male with Multiple Hyperpigmented Macules on Trunk
Years Old Male with Multiple Hyperpigmented Macules on Trunk
 Gray Pigmented Macule on Right Cheek
Gray Pigmented Macule on Right Cheek
 6 Years Old Male with Multiple Black Spots on Face
6 Years Old Male with Multiple Black Spots on Face
 of Skin Pigmentation on Feet in a Female
of Skin Pigmentation on Feet in a Female
 Young Man with Hypopigmented Macules on Trunk and Multiple Shiny Nodules Over Face
Young Man with Hypopigmented Macules on Trunk and Multiple Shiny Nodules Over Face
 Young Boy with Generalized Hyperpigmentation
Young Boy with Generalized Hyperpigmentation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


