Key Points
- ▪
Following injury to the lymphatic system, development of lymphedema involves a predictable progression of disease represented by histological, architectural, and pressure gradient changes within the involved area.
- ▪
In addition to the local site of lymphedema, changes to the entire lymphatic system must be considered in order to achieve consistent outcomes following lymphatic microsurgery.
- ▪
Understanding the progression of disease provides a foundation for decision-making in selecting the anatomical site of intervention and type of microsurgical procedure.
- ▪
Timing of surgical intervention may help dictate the type of surgical procedure, the optimal recipient site, and the likely achievable outcome.
Introduction
Reconstructive microsurgery for lymphedema is rising in popularity. Traditional algorithms for lymphedema treatment are now being modified to include complex microsurgical procedures. The field of reconstructive microsurgery has rapidly experienced innovation and technical improvements based mainly on arterial and venous systems, and skin/muscle anatomy and perfusion. Lymphatic microsurgery represents a unique discipline with unique physiologic considerations. Investigators in the field of lymphology and lymphedema-related disorders have formed the foundation for surgical procedures addressing lymphedema. In particular, outcomes following microsurgical procedures have been variable among selective centers around the world, yet certain groups have been able to demonstrate reproducible outcomes using their techniques. Although technical considerations may account for some degree of variation, a lack of an in-depth understanding of the dynamic aspect of the lymphatic system may further explain this variability.
The lymphatic system is an embryologic derivative of the venous system therefore it shares some physiologic similarities. However, important differences in vascular and lymphatic systems are crucial and need to be understood clearly when considering lymphatic microsurgery. In primary or congenital cases of lymphedema, special consideration for the absence and/or dysfunction of each component of the system will allow appropriate surgical decision-making in these unique cases. In secondary lymphedema, which represents the majority of cases in industrialized countries, disruptive physiologic changes occur in a characteristic manner. The purpose of this chapter is to highlight and emphasize the guiding principles of lymphatic pathophysiology and its application to microsurgery to allow clinicians to optimize their decision-making processes and to achieve reproducible outcomes.
Disease Progression and Lymphatic Ultrastructural Changes
Similar to other disease entities throughout the body, the clinical manifestation and presentation of symptoms occur following a significant degree of chronic injury. In the setting of secondary lymphedema, lymphadenectomy and lymphatic injury is the initial insult. Following injury (surgery, radiation, chemotherapy, and/or trauma), healing or regeneration of damaged lymphatics may occur with variable success. Spontaneous healing and the regenerative capacity of native tissues are further limited when neoadjuvant or adjuvant radiation therapy is incorporated in treatment.
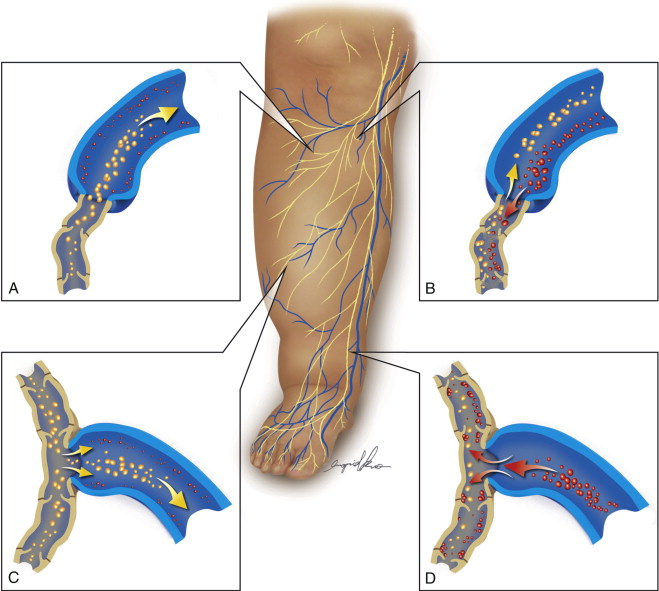
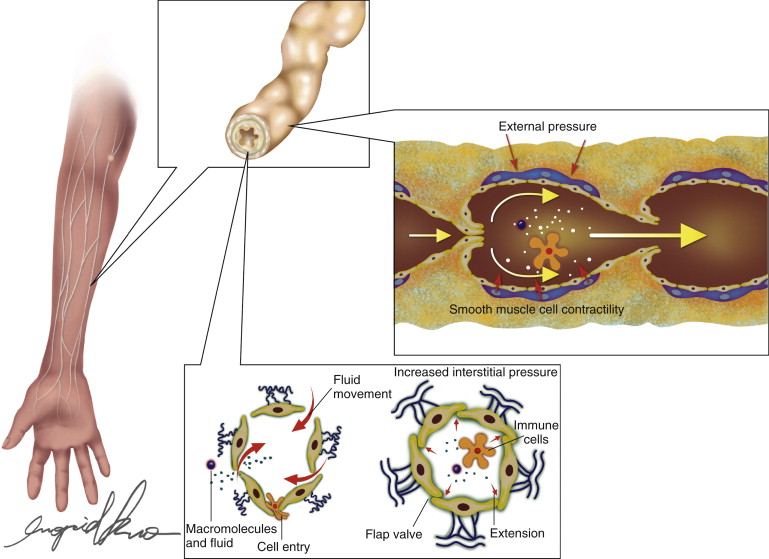
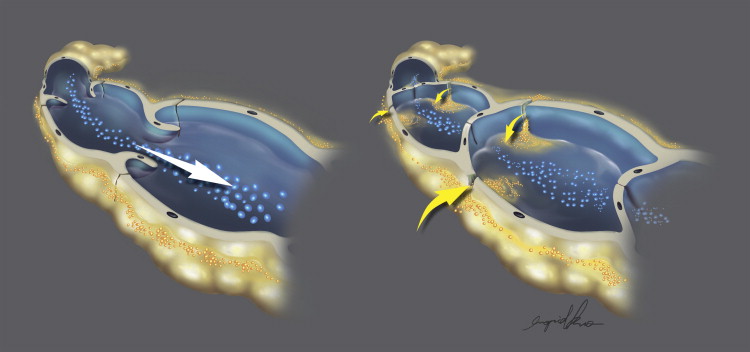
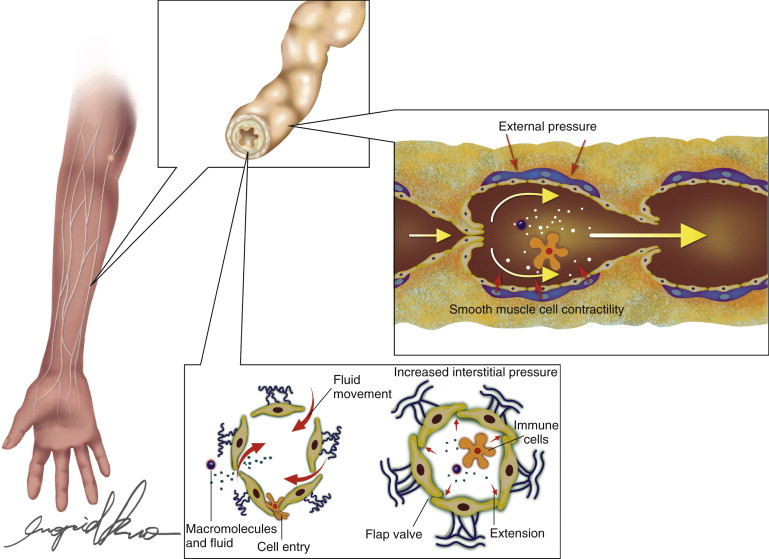
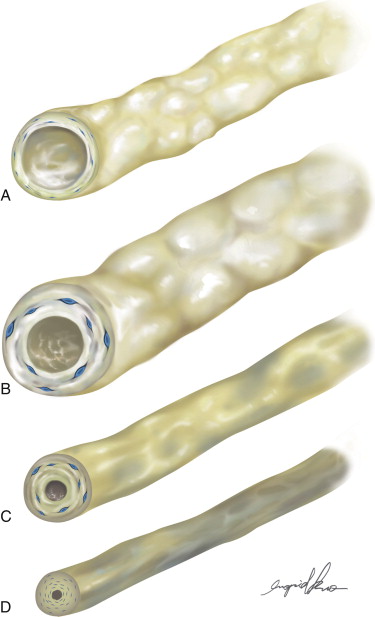
Following the initial injury or disruption of the physiologic lymph flow, a cascade of events occurs prior to developing clinically evident lymphedema. In the normal physiologic state, lymphatic fluid is propelled along an extremity via an active pumping mechanism (composed of smooth muscle cells) of the collecting and precollecting ducts combined with the concerted action of unidirectional valves ( Figure 8.1 ). Synchronized lymphangion (the functional lymphatic unit) contraction further contributes to centripetal negative pressure augmenting a systemic propulsion of unidirectional flow. In fact, propulsion of lymph has been described to occur in peristaltic waves with increasing frequency of contraction as lymphatic intraluminal pressure increases ( Figure 8.2 ). Proximal insult leads to impaired egress of lymph fluid from the site of injury and increases lymphatic fluid impedance resulting in lymphatic hypertension. The changes that follow this lymphodynamic condition result in characteristic pathology ( Figure 8.3 ). As increased intraluminal pressure persists, lymphatic vessel dilation progresses to a state of pathologic ectasia. This leads to irreversible valve insufficiency, and a subsequent architectural breakdown of intraluminal valves continues with remodeling of smooth muscle cells and connective tissue of the extraluminal lymphatics and diminishes one-way functional of lymph movement. The lymph flow at this stage is bidirectional, which may be amenable to extrinsic forces such as gravity, muscular contraction, compression therapy, and is responsive to intraluminal pressure gradients. As a compensatory mechanism, smooth muscle cells along the walls of lymphatics hypertrophy and neighboring cells will assume phenotypic attributes similar to contractile smooth muscle cells. The hypertrophic process further ensues with eventual lumen obliteration resulting in regurgitant lymph flow in the subdermal lymphatic ducts. Once subdermal lymphatic ducts are overwhelmed, lymph extravasation will lead to clinical signs of lymphedema ( Figure 8.3 ). Progression of these events in the setting of clinical lymphedema may differ from patient to patient, but the sequence of events occurs in a predictable fashion.
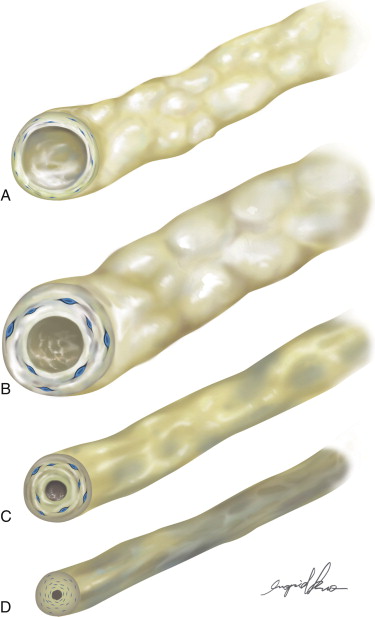
A histologic evaluation of lymphatic ducts reveals ultrastructural changes that occur in a predictable and characteristic fashion. Interestingly, a heterogeneity of diseased lymphatic ducts are present within individual patients, suggesting that ultrastructural changes to the lymphatics occur in concert with the progression of disease. A higher density of advanced histologic changes is found to be present in more clinically advanced patients. These results highlight the observation that an individual patient will likely have diseased lymphatic ducts at varying stages of severity.
Changes to the lymphatic architecture are also evident on lymphographic studies that support histologic findings and elucidate the concept of a progression from subclinical to clinically evident lymphedema. Bidirectional flow, static networks of dye in the distal portion of extremities, and accumulation of dye at the injection site have been observed in asymptomatic, considered at-risk patients, and symptomatic patients revealing the chronic changes that ensue following an insult to proximal lymphatics. Imaging provides a dynamic method of visualizing the lymphatic vascular network and indocyanine green (ICG) diffusion patterns have been characterized based on disease severity as well. Ultimately, lymphatic insufficiency evolves into a chronic pathologic process resulting in deterioration of individual lymphatic ducts, which results in a higher density of stenosed and obliterated duct lumens. Once dependent edema is clinically evident, one can infer that the structural changes described above have already occurred.
Disease Progression and Lymphatic Ultrastructural Changes
Similar to other disease entities throughout the body, the clinical manifestation and presentation of symptoms occur following a significant degree of chronic injury. In the setting of secondary lymphedema, lymphadenectomy and lymphatic injury is the initial insult. Following injury (surgery, radiation, chemotherapy, and/or trauma), healing or regeneration of damaged lymphatics may occur with variable success. Spontaneous healing and the regenerative capacity of native tissues are further limited when neoadjuvant or adjuvant radiation therapy is incorporated in treatment.
Following the initial injury or disruption of the physiologic lymph flow, a cascade of events occurs prior to developing clinically evident lymphedema. In the normal physiologic state, lymphatic fluid is propelled along an extremity via an active pumping mechanism (composed of smooth muscle cells) of the collecting and precollecting ducts combined with the concerted action of unidirectional valves ( Figure 8.1 ). Synchronized lymphangion (the functional lymphatic unit) contraction further contributes to centripetal negative pressure augmenting a systemic propulsion of unidirectional flow. In fact, propulsion of lymph has been described to occur in peristaltic waves with increasing frequency of contraction as lymphatic intraluminal pressure increases ( Figure 8.2 ). Proximal insult leads to impaired egress of lymph fluid from the site of injury and increases lymphatic fluid impedance resulting in lymphatic hypertension. The changes that follow this lymphodynamic condition result in characteristic pathology ( Figure 8.3 ). As increased intraluminal pressure persists, lymphatic vessel dilation progresses to a state of pathologic ectasia. This leads to irreversible valve insufficiency, and a subsequent architectural breakdown of intraluminal valves continues with remodeling of smooth muscle cells and connective tissue of the extraluminal lymphatics and diminishes one-way functional of lymph movement. The lymph flow at this stage is bidirectional, which may be amenable to extrinsic forces such as gravity, muscular contraction, compression therapy, and is responsive to intraluminal pressure gradients. As a compensatory mechanism, smooth muscle cells along the walls of lymphatics hypertrophy and neighboring cells will assume phenotypic attributes similar to contractile smooth muscle cells. The hypertrophic process further ensues with eventual lumen obliteration resulting in regurgitant lymph flow in the subdermal lymphatic ducts. Once subdermal lymphatic ducts are overwhelmed, lymph extravasation will lead to clinical signs of lymphedema ( Figure 8.3 ). Progression of these events in the setting of clinical lymphedema may differ from patient to patient, but the sequence of events occurs in a predictable fashion.
A histologic evaluation of lymphatic ducts reveals ultrastructural changes that occur in a predictable and characteristic fashion. Interestingly, a heterogeneity of diseased lymphatic ducts are present within individual patients, suggesting that ultrastructural changes to the lymphatics occur in concert with the progression of disease. A higher density of advanced histologic changes is found to be present in more clinically advanced patients. These results highlight the observation that an individual patient will likely have diseased lymphatic ducts at varying stages of severity.
Changes to the lymphatic architecture are also evident on lymphographic studies that support histologic findings and elucidate the concept of a progression from subclinical to clinically evident lymphedema. Bidirectional flow, static networks of dye in the distal portion of extremities, and accumulation of dye at the injection site have been observed in asymptomatic, considered at-risk patients, and symptomatic patients revealing the chronic changes that ensue following an insult to proximal lymphatics. Imaging provides a dynamic method of visualizing the lymphatic vascular network and indocyanine green (ICG) diffusion patterns have been characterized based on disease severity as well. Ultimately, lymphatic insufficiency evolves into a chronic pathologic process resulting in deterioration of individual lymphatic ducts, which results in a higher density of stenosed and obliterated duct lumens. Once dependent edema is clinically evident, one can infer that the structural changes described above have already occurred.
Venous Shunting of Lymphatic Fluid
Lymphovenous bypass (LVB), shunting, and anastomosis (LVA) are all terms that describe artificial drainage of lymphatic fluid into the venous system. Lymphovenous shunting techniques will provide decompression of the lymphatic system if performed correctly. In addition to the technical complexities of these procedures, a thorough understanding of how to utilize the diseased lymphatic system to maximize the lymphatic outflow is necessary to achieve reproducible outcomes.
Early experience with these initial techniques of diverting lymphatic flow into an adjacent vein suggested temporary improvement with eventual failure of anastomotic techniques. Since these early interventions, more rigorous evaluation, technical improvements, and expanding clinical experience has led to improved results and reproducible outcomes. In addition to improvement in surgical techniques, the implementation of live lymphodynamic evaluation using ICG lymphography, and near-infrared (NIR) fluoroscopy provides a method for dynamic mapping and monitoring of the superficial lymphatic system. These innovative tools are easier to implement than traditional lymphoscintigraphy and have greatly contributed to the successful reproducibility of lymphovenous shunting techniques and their subsequent outcomes.
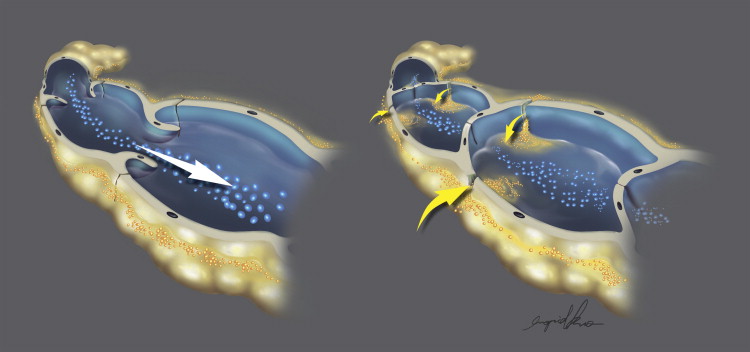
A combination of physiologic conditions is required to successfully perform a functional lymphovenous shunting procedure. Focusing on the lymphatic vessel, an early stage disease will exhibit normal vessel architecture with preserved propulsive lymphatic flow. Selecting venous shunting techniques in these patients requires exploiting the inherent pumping mechanism in concert with intact valvular competence of the lymphangion. The lymphovenous anastomotic technique will result in decompression of the elevated pressures of the distal lymphatic, although proximal intraluminal insufficiency may or may not have already developed in the patient’s current disease state. The importance of this fact should determine whether to perform a side-to-end or end-to-end anastomosis and should dictate the location of the shunting procedure ( Figure 8.4 ).