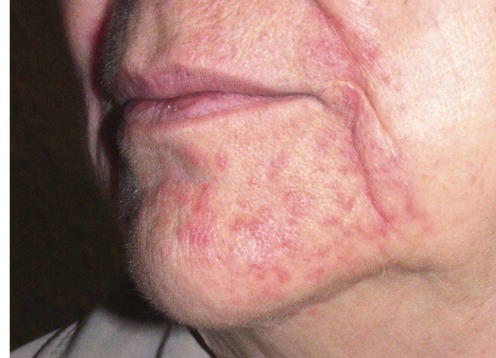
179 Perioral dermatitis Antonios Kanelleas and John Berth-Jones Evidence Levels: A Double-blind study B Clinical trial ≥ 20 subjects C Clinical trial < 20 subjects D Series ≥ 5 subjects E Anecdotal case reports Perioral dermatitis is a persistent erythematous eruption of inflammatory papules (and sometimes pustules) on the chin, perioral areas, and nasolabial folds, characteristically sparing the skin immediately adjacent to the vermilion border. The main symptoms include pruritus, burning sensation and soreness. It is usually seen in young women, but also occurs in childhood. The etiology is unknown, however the development of perioral dermatitis is frequently preceded by intentional or inadvertent application of potent topical corticosteroids to the facial skin. The use of steroid inhalers may also induce perioral dermatitis. A similar eruption involving the eyelids and periorbital skin has been termed periocular dermatitis. The granulomatous subset of perioral dermatitis, which is seen in prepubertal children, presents with small flesh-colored or yellow-brown papules. The suggested relationship of perioral dermatitis with infectious agents and infestations such as Candida spp, Demodex folliculorum and fusiform bacteria has not been confirmed. However, a high prevalence of atopy has been found amongst patients with perioral dermatitis. Although sometimes described as a variant of rosacea, perioral dermatitis is distinguished from this disease by its distribution, by the relatively monomorphic appearance of the lesions, by the absence of flushing and telangiectasia, and by its tendency to occur in younger patients. Differential diagnoses also include contact dermatitis, which does not usually spare the lip margins. Management strategy Many cases are associated with the use of potent topical corticosteroids, and withdrawal of this medication is the most important measure in this group. Any cosmetic products applied on the area should also be discontinued. Patients must be warned that the condition may initially flare after this maneuvre. If the flare proves intolerable, initial use of a less potent topical corticoid can often be helpful. Systemic tetracyclines are also frequently employed, and a range of other modalities are used less frequently. In most cases there will be a permanent remission, but relapses may rarely occur. In case of treatment failure, contact dermatitis should be excluded by patch testing. Specific investigations No investigation is routinely required First-line treatment Withdrawal of topical corticoids B Oral tetracyclines B Complications of topical hydrocortisone. Guin JD. J Am Acad Dermatol 1981; 4: 417–22. Perioral dermatitis developed following the use of topical hydrocortisone. Although usually associated with the use of potent topical corticosteroids, this case suggests that even hydrocortisone may induce perioral dermatitis. Only gold members can continue reading. Log In or Register to continue Share this: Click to share on X (Opens in new window) X Click to share on Facebook (Opens in new window) Facebook Related Related posts: Cat scratch disease Hemangiomas Tinea capitis Herpes genitalis Necrolytic migratory erythema Nevoid basal cell carcinoma syndrome Stay updated, free articles. Join our Telegram channel Join Tags: Treatment of Skin Disease Comprehensive Therapeutic Strategies Aug 7, 2016 | Posted by admin in Dermatology | Comments Off on Perioral dermatitis Full access? Get Clinical Tree Get Clinical Tree app for offline access Get Clinical Tree app for offline access
179 Perioral dermatitis Antonios Kanelleas and John Berth-Jones Evidence Levels: A Double-blind study B Clinical trial ≥ 20 subjects C Clinical trial < 20 subjects D Series ≥ 5 subjects E Anecdotal case reports Perioral dermatitis is a persistent erythematous eruption of inflammatory papules (and sometimes pustules) on the chin, perioral areas, and nasolabial folds, characteristically sparing the skin immediately adjacent to the vermilion border. The main symptoms include pruritus, burning sensation and soreness. It is usually seen in young women, but also occurs in childhood. The etiology is unknown, however the development of perioral dermatitis is frequently preceded by intentional or inadvertent application of potent topical corticosteroids to the facial skin. The use of steroid inhalers may also induce perioral dermatitis. A similar eruption involving the eyelids and periorbital skin has been termed periocular dermatitis. The granulomatous subset of perioral dermatitis, which is seen in prepubertal children, presents with small flesh-colored or yellow-brown papules. The suggested relationship of perioral dermatitis with infectious agents and infestations such as Candida spp, Demodex folliculorum and fusiform bacteria has not been confirmed. However, a high prevalence of atopy has been found amongst patients with perioral dermatitis. Although sometimes described as a variant of rosacea, perioral dermatitis is distinguished from this disease by its distribution, by the relatively monomorphic appearance of the lesions, by the absence of flushing and telangiectasia, and by its tendency to occur in younger patients. Differential diagnoses also include contact dermatitis, which does not usually spare the lip margins. Management strategy Many cases are associated with the use of potent topical corticosteroids, and withdrawal of this medication is the most important measure in this group. Any cosmetic products applied on the area should also be discontinued. Patients must be warned that the condition may initially flare after this maneuvre. If the flare proves intolerable, initial use of a less potent topical corticoid can often be helpful. Systemic tetracyclines are also frequently employed, and a range of other modalities are used less frequently. In most cases there will be a permanent remission, but relapses may rarely occur. In case of treatment failure, contact dermatitis should be excluded by patch testing. Specific investigations No investigation is routinely required First-line treatment Withdrawal of topical corticoids B Oral tetracyclines B Complications of topical hydrocortisone. Guin JD. J Am Acad Dermatol 1981; 4: 417–22. Perioral dermatitis developed following the use of topical hydrocortisone. Although usually associated with the use of potent topical corticosteroids, this case suggests that even hydrocortisone may induce perioral dermatitis. Only gold members can continue reading. Log In or Register to continue Share this: Click to share on X (Opens in new window) X Click to share on Facebook (Opens in new window) Facebook Related Related posts: Cat scratch disease Hemangiomas Tinea capitis Herpes genitalis Necrolytic migratory erythema Nevoid basal cell carcinoma syndrome Stay updated, free articles. Join our Telegram channel Join Tags: Treatment of Skin Disease Comprehensive Therapeutic Strategies Aug 7, 2016 | Posted by admin in Dermatology | Comments Off on Perioral dermatitis Full access? Get Clinical Tree

 Withdrawal of topical corticoids
Withdrawal of topical corticoids Oral tetracyclines
Oral tetracyclines


