Lorch-Dauk KC, Comrov E, Blumer JL, O’Riordan MA, Furman LM. Clin Pediatr 2010; 49: 280–6.
Tinea capitis
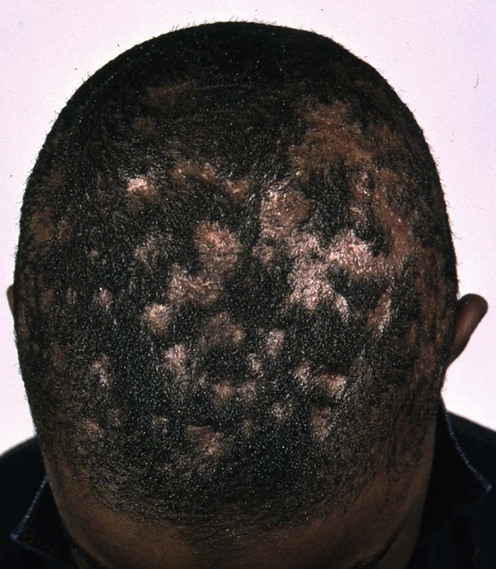
Specific investigations
Tinea capitis: predictive value of symptoms and time to cure with griseofulvin treatment.
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree





