Treatment of the aging lower eyelid is determined by the anatomic variables noted for each surgical candidate. Although surgeons have traditionally considered dermatochalasis, fat pseudoherniation, and eyelid position as the main treatment objectives in lower blepharoplasty, the vector of the infraorbital rim and the anterior plane of the cornea, tear trough, and aging in the midface also merit critical consideration. In this article, indications and technical aspects, the transconjunctival and external approaches, fat excision versus fat repositioning, and suborbicularis oculi fat lifting and fat transplantation are discussed and the authors’ preference for the various methods of lower blepharoplasty is presented. Common adjunct procedures used to supplement lower blepharoplasty techniques and the role of injectable fillers in periocular rejuvenation are also mentioned.
Lower eyelid rejuvenation requires careful consideration of all layers of the eyelid and the transition to the midface. Hereditary anatomic variations in these structures and the changes typically observed with aging must be considered in optimizing periocular treatment outcomes. In the preoperative period, a thorough periocular examination is critical in determining optimal treatment strategies. The patient’s medical history, expectations, and motivations must also be clearly defined before further surgical planning. Fat pseudoherniation, dermatochalasis, orbicularis hypertrophy, and prominent tear trough deformity are the most common indications for lower eyelid rejuvenation. Most commonly, fat pseudoherniation and prominence of the tear trough are addressed through lower eyelid blepharoplasties using either transcutaneous or transconjunctival techniques, with or without fat repositioning. Suborbicularis oculi fat (SOOF) lifting and fat transplantation have also been described as methods for softening the prominent tear trough in select cases. The indications and methods for each approach are described, with particular attention dedicated to the senior author’s (KAL) technique for transconjunctival lower eyelid blepharoplasty with orbital fat repositioning, the most commonly indicated lower eyelid procedure in the author’s experience. Adjunctive procedures for skin resurfacing and the utility of tear trough augmentation with fillers are also briefly described.
Anatomic changes with aging
The periorbital area demonstrates some of the earliest signs of facial aging. The integrity of the septum diminishes with advancing age such that orbital fat pseudoherniation leads to the appearance of bags or fullness in the lower eyelid. With advancing age, increased laxity in the structurally supportive tissues of the orbit also leads to relative settling of the globe, further exacerbating fat pseudoherniation through the areas of septal weakening. Laxity in the lower eyelid septum can also be hereditary, as evidenced by the appearance of fat pseudoherniation in many adolescents and young adults. Orbital fat pseudoherniation contributes to the observed deepening of the nasojugal fold, or tear trough, that is associated with aging and gives the eyes a more fatigued, haggard appearance.
Below the tear trough and orbital rim, the fatty tissues of the midface and cheek lose volume and descend as aging progresses. In a similar fashion, the SOOF loses volume and descends over time. In a youthful face, cadaveric studies have demonstrated that the SOOF attaches to the arcus marginalis at the level of the inferior orbital rim. With aging, SOOF descent and volume loss contribute to deepening of the tear trough deformity and lengthening of the lower eyelid. Concurrently, the orbicularis oculi muscle of the lower eyelid can hypertrophy, leading to heaviness, sagging, and deeper rhytids in the lower eyelid. These changes in midfacial fat, SOOF, and orbicularis oculi contribute to the increasing potential for eyelid malposition, deepening of the tear trough, and rounding of the eye. Lower eyelid skin also progressively loses its elasticity with aging, leading to progressive dermatochalasis with fine and deep rhytids.
Preoperative evaluation
General Considerations
A complete discussion of all preoperative considerations for periocular rejuvenation procedures is beyond the scope of this article. Nevertheless, any history of dry eye symptoms, prior orbital or eye procedures, and comorbid conditions (ie Graves ophthalmopathy) or medications that can alter anticipated outcomes or wound healing should be investigated. Preoperative examination should address visual acuity, extraocular muscle function, tear film adequacy, lower eyelid tone, and lower eyelid resting position. Eyelid malposition or excessive laxity noted preoperatively should always be addressed before or concurrently with elective procedures. A frank discussion regarding motivations, surgical risks, and anticipated benefits for proposed procedures must also take place between the surgeon and the patient, because inappropriate motivations, unrealistic expectations, and conditions that alter a patient’s self-perception can preclude surgical candidacy.
Position of the Globe and the Inferior Orbital Rim
The relative positions of the globe and inferior orbital rim should always be assessed preoperatively, because their relationship is critical in determining the optimal procedures for treatment of the aging lower eyelid and tear trough deformity. In the sagittal plane, if the anterior margin of the inferior orbital rim is posterior to the anterior-most point of the cornea, then the patient has a negative vector anatomy in the malar position relative to the anterior surface of the globe ( Fig. 1 ). Patients with a negative vector anatomy are more likely to have preoperative scleral show, because they usually have some degree of midfacial hypoplasia. Preoperative scleral show should prompt evaluation of the position of the inferior orbital rim relative to the globe, because simple excision of the pseudoherniating lower eyelid fat in patients with negative vector anatomy often leads to exacerbation of the tear trough deformity and can lead to increased scleral show. Given these anatomic considerations, patients with negative vector anatomy with fat pseudoherniation are excellent candidates for lower eyelid blepharoplasties with fat repositioning.
If the anterior margin of the globe has the same projection as the inferior orbital rim, the patient has neutral vector anatomy. In the senior author’s experience, patients with neutral vector anatomy with fat pseudoherniation and tear trough deformities are also ideally suited for lower blepharoplasties with fat repositioning, because the repositioning minimizes the risk of future orbital hollowing and deepening of the tear trough deformity, seen with aggressive simple fat excision.
In contrast, patients seeking periocular rejuvenation with fat pseudoherniation and an inferior orbital rim positioned anterior to the anterior-most point of the cornea are not ideal candidates for orbital fat repositioning. In such candidates with positive vector anatomy, conservative excision of fat is recommended when pseudoherniating fat is noted, because repositioning of orbital fat over the orbital rim may actually exaggerate, rather than improve, the already sunken appearance of the globe. In candidates with positive vector anatomy with tear trough deformity and little or no significant fat pseudoherniation, volume augmentation of the tear trough with fat transplantation, SOOF lifting, or filler augmentation is recommended.
Malar Bags
Focal areas of malar edema, or malar bags, should also be noted and discussed specifically with the patient in the preoperative setting. Malar bags can be a source of frustration for patients and surgeons. Surgical candidates should be advised that there is little consensus as to the most effective treatment for malar bags. The candidates should also be advised that sufficient improvement in lower eyelid fat pseudoherniation and dermatochalasis usually does not significantly alter the appearance of malar bags, even with extended skin or skin muscle flap techniques. In these patients, the surgeon should advise that the malar bags may actually become more noticeable once the lower eyelid concerns have been addressed ( Fig. 2 ).
Preoperative evaluation
General Considerations
A complete discussion of all preoperative considerations for periocular rejuvenation procedures is beyond the scope of this article. Nevertheless, any history of dry eye symptoms, prior orbital or eye procedures, and comorbid conditions (ie Graves ophthalmopathy) or medications that can alter anticipated outcomes or wound healing should be investigated. Preoperative examination should address visual acuity, extraocular muscle function, tear film adequacy, lower eyelid tone, and lower eyelid resting position. Eyelid malposition or excessive laxity noted preoperatively should always be addressed before or concurrently with elective procedures. A frank discussion regarding motivations, surgical risks, and anticipated benefits for proposed procedures must also take place between the surgeon and the patient, because inappropriate motivations, unrealistic expectations, and conditions that alter a patient’s self-perception can preclude surgical candidacy.
Position of the Globe and the Inferior Orbital Rim
The relative positions of the globe and inferior orbital rim should always be assessed preoperatively, because their relationship is critical in determining the optimal procedures for treatment of the aging lower eyelid and tear trough deformity. In the sagittal plane, if the anterior margin of the inferior orbital rim is posterior to the anterior-most point of the cornea, then the patient has a negative vector anatomy in the malar position relative to the anterior surface of the globe ( Fig. 1 ). Patients with a negative vector anatomy are more likely to have preoperative scleral show, because they usually have some degree of midfacial hypoplasia. Preoperative scleral show should prompt evaluation of the position of the inferior orbital rim relative to the globe, because simple excision of the pseudoherniating lower eyelid fat in patients with negative vector anatomy often leads to exacerbation of the tear trough deformity and can lead to increased scleral show. Given these anatomic considerations, patients with negative vector anatomy with fat pseudoherniation are excellent candidates for lower eyelid blepharoplasties with fat repositioning.
If the anterior margin of the globe has the same projection as the inferior orbital rim, the patient has neutral vector anatomy. In the senior author’s experience, patients with neutral vector anatomy with fat pseudoherniation and tear trough deformities are also ideally suited for lower blepharoplasties with fat repositioning, because the repositioning minimizes the risk of future orbital hollowing and deepening of the tear trough deformity, seen with aggressive simple fat excision.
In contrast, patients seeking periocular rejuvenation with fat pseudoherniation and an inferior orbital rim positioned anterior to the anterior-most point of the cornea are not ideal candidates for orbital fat repositioning. In such candidates with positive vector anatomy, conservative excision of fat is recommended when pseudoherniating fat is noted, because repositioning of orbital fat over the orbital rim may actually exaggerate, rather than improve, the already sunken appearance of the globe. In candidates with positive vector anatomy with tear trough deformity and little or no significant fat pseudoherniation, volume augmentation of the tear trough with fat transplantation, SOOF lifting, or filler augmentation is recommended.
Malar Bags
Focal areas of malar edema, or malar bags, should also be noted and discussed specifically with the patient in the preoperative setting. Malar bags can be a source of frustration for patients and surgeons. Surgical candidates should be advised that there is little consensus as to the most effective treatment for malar bags. The candidates should also be advised that sufficient improvement in lower eyelid fat pseudoherniation and dermatochalasis usually does not significantly alter the appearance of malar bags, even with extended skin or skin muscle flap techniques. In these patients, the surgeon should advise that the malar bags may actually become more noticeable once the lower eyelid concerns have been addressed ( Fig. 2 ).
Procedures
Lower Eyelid Blepharoplasty
Candidates for lower eyelid blepharoplasty should demonstrate lower eyelid fat pseudoherniation with or without orbicularis hypertrophy, excess lower eyelid skin, the appearance of circles under the eyes, or prominent depth in the tear trough deformity. Candidates presenting without significant lower eyelid fat pseudoherniation and a prominent tear trough deformity require fat transplantation, filler augmentation, or SOOF lifting. Having the patient gaze upward exaggerates bulging in the lower eyelid secondary to fat pseudoherniation. Once the presence of significant fat pseudoherniation has been established, the surgeon must decide on whether to use transconjunctival or transcutaneous techniques and to recommend orbital fat excision or fat repositioning.
Transconjunctival techniques
With the exception of considerable dermatochalasis or orbicularis oculi hypertrophy, transconjunctival techniques work well for most lower eyelid blepharoplasty procedures. Transconjunctival approaches are associated with lower incidences of postoperative lower eyelid retraction and obviate any potential for external scar. Especially in cases of preoperative scleral show, transconjunctival approaches are recommended, because the release of the lower eyelid retractors during this approach theoretically allows for elevation of the lower eyelid position relative to the globe. Transconjunctival approaches are also ideally suited for young patients with familial development of lower lid fat pseudoherniation, because they rarely have significant dermatochalasis or orbicularis hypertrophy that requires surgical reduction. These patients are also excellent candidates for fat excision as opposed to fat repositioning. Although transcutaneous scars can be very inconspicuous, the risk of postoperative scar depigmentation (white scars) also leads many surgeons to recommend transconjunctival techniques in individuals with darker skin types (Fitzpatrick skin types V and VI).
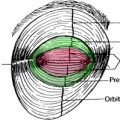
Transconjunctival approaches proceed in either the preseptal or retroseptal plane ( Fig. 3 ). No consensus as to the best technique was noted in the authors’ literature review. Proponents of the preseptal method report that disruption of the orbicularis–orbital septum fascial connections leads to further scar tissue formation on the septum, which bolsters against the pressures of fat pseudoherniation postoperatively. Retroseptal method proponents argue that separating the orbital septum from the orbicularis in the preseptal method creates a cicatricial plane that can potentially result in inferior traction on the lid and postoperative lid malposition. In the senior author’s experience, eyelid malposition with either transconjunctival method is rare.