This article discusses the anatomy of the periocular region in terms of how the parts interact and what happens anatomically with aging. Detailed function of the anatomic area is also presented. Periocular anatomy, the lacrimal system, and orbital anatomy are first discussed, followed by characteristics of aging.
Eyelid anatomy is one of the more complex sets of anatomic relationships in the face. Differences are measured in millimeters, and structures are extremely fine and delicate ( Fig. 1 ). The tissue can be very difficult to work with, requiring the utmost attention to detail. It is imperative to have an understanding of the complex anatomy and function of this region before any surgical or nonsurgical adventure is undertaken.
Anatomic descriptions involve western aesthetic tenets in Caucasians unless otherwise specified; although, as there are ever-increasing variations in aesthetic goals and many varying ethnicities, there is some generalization. The function of the lacrimal system and the orbital contents are beyond the scope of this article and are addressed only as they pertain to nonophthalmologic procedures.
Periorbital anatomy
Lid Topography
A few anatomic relationships are important when evaluating the orbital region. First, brow position may be evaluated. Common aesthetic relationships differ. In men, the brow is often most pleasing at the superior orbital rim in a less arched position. In women, the brow is ideally described as club-shaped, beginning in line with the alar creases medially at the orbital rim and arching above the rim with the apex over the lateral limbus and descending back down to the level of the orbital rim.
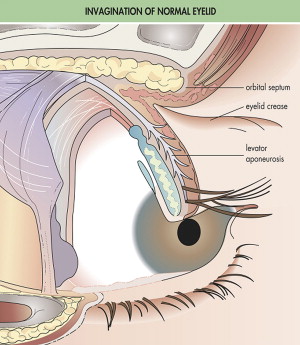
The upper lid crease is formed by the insertion of the levator aponeurotic fibers into the skin ( Fig. 2 ). The crease is usually 8 to 9 mm in men and 9 to 12 mm in women. In the Asian population, the insertion is significantly closer to the lid margin, resulting in a lower or absent crease. The lower lid fold may be 3 mm from the lid margin and is more common in the pediatric population ( Fig. 3 ).
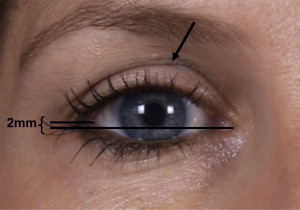
The palpebral fissure is 28 to 30 mm wide and 9 to 10 mm high, with the lateral canthal angle 2 mm higher on a horizontal plane than the medial canthus (3 mm in the Asian population). The lateral canthal angle is 30° to 40°. The medial canthus lies about 15 mm from the midline (see Fig. 3 ).
The upper lid margin lies from the level of the superior limbus to 2 mm below normally. Upper lid excursion may average 12 mm, whereas lower lid excursion is 5 mm.
Lid Anatomy
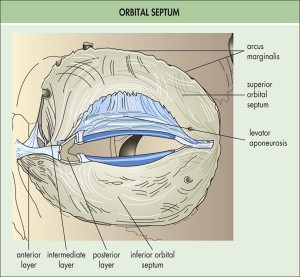
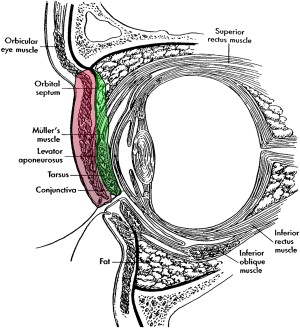
The eyelids are constructed with 3 anatomic and surgical layers: anterior, middle, and posterior lamellae ( Figs. 4 and 5 ). The anterior lamella is composed of the skin, subcutaneous tissue, and orbicularis muscle. The skin is often less than 1 mm thick and may be thin enough to reveal underlying vessels and discoloration. Beneath the skin, there is some loose connective tissue in the preseptal and preorbital regions, which is absent in the pretarsal area. This subcutaneous tissue allows for the easy separation of the skin and muscle during surgical dissection.
The deepest layer of the anterior lamella is the orbicularis oculi muscle, which is divided into 3 regions ( Fig. 6 ). The orbital portion overlaps with other muscles of facial expression and may contribute to festoons of the lower lid in the aging process. The origin of this part of the muscle is the medial orbital margin and the medial palpebral ligament, with the insertion being lateral cheek skin.
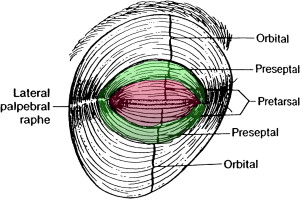
The palpebral or preseptal portion is over the orbital septum, and the origin and insertion are the medial palpebral ligament and lateral palpebral raphe, respectively (see Fig. 6 ). The pretarsal region of the orbicularis muscle overlies the tarsal plate ( Fig. 7 ). Beneath the orbicularis oculi muscle is the submuscular areolar tissue. Superiorly, this tissue may be followed to terminate at the retro-orbicularis oculi fat and inferiorly may be followed to the suborbicularis oculi fat.
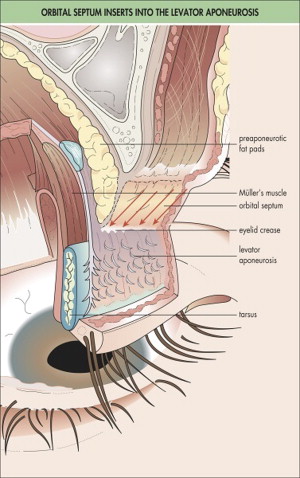
The posterior lamella of the upper lid is more complex mostly because of the insertions of the levator aponeurosis (see Fig. 2 ). The deepest layer of the upper and lower lid posterior lamella is the conjunctiva. The conjunctiva is a thin epithelial mucosal membrane lining the inner lid and adheres to the tarsal plate. The tarsal plate is the area of dense fibrous tissue that gives the lid it’s strength and rigidity. It is about 29 mm long and 1 mm thick. They attach to the medial and lateral palpebral ligaments (see Fig. 7 ).
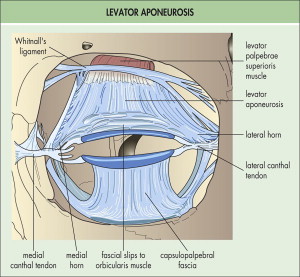
The levator aponeurosis is the most superficial portion of the posterior lamella. It invests with the levator palpebrae superioris muscle, spreads laterally and medially, and attaches to the orbital septum forming the lid crease (see Fig. 3 ). Muller muscle, which has sympathetic innervation, lies beneath the levator and is an upper lid retractor as well.
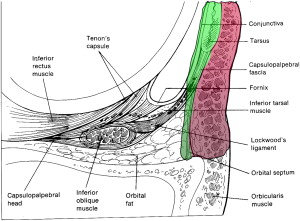
The posterior lamella of the lower lid is similar to that of the upper lid with respect to the conjunctiva and tarsal plate. The conjunctiva is identical to that of the upper lid. The lower tarsal plate is shorter in height than the upper tarsal plate and is 3.5 to 5 mm high (see Fig. 7; Fig. 8 ).