Figure 13.1
Pemphigus foliaceus (var.) herpetiformis: (a, b) grouped vesicles, bullae and crusts over erythematous and edematous plaques on torso and (c) dorsal aspect of the feet, (d) and (e) pruritic vesicles on the trunk and sparse lesions on the inferior limbs (f) and (g)
Based on the case description and the photograph, what is your diagnosis?
1.
Pemphigus foliaceus
2.
Pemphigus herpetiformis
3.
Dermatitis herpetiformis
4.
Bullous pemphigoid
5.
Linear IgA bullous dermatosis
After a negative Tzanck smear, a new biopsy was performed, and histopathology analysis showed eosinophilic spongiosis (Fig. 13.2). Immunological studies (Fig. 13.3) revealed intercellular, intraepidermal deposits of IgG and C3, circulating IgG antibodies (titer 1:320) and maintenance of positive ELISA index for desmoglein 1 (45), consistent with the diagnosis of pemphigus herpetiformis. Prednisone was increased to 30 mg/day, associated to sulfamethoxypyridazine (1 g/day). Lesions rapidly improved after 5 weeks, allowing corticosteroid and sulphonamide discontinuation after 3 months. She presented new lesions 1 month after therapy was withdrawn, and prednisone 40 mg/day and sulfamethoxypyridazine 1 g/day were reintroduced. Partial remission occurred after 4 months, and due to sporadic erythematous, pruritic papules and plaques on the trunk, sulphonamide was administered to the patient for 10 years.
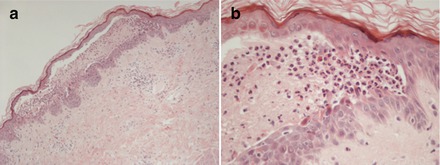
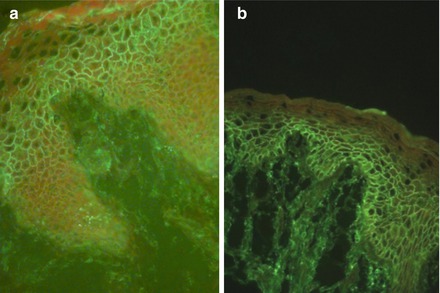
Figure 13.2
Pemphigus foliaceus (var.) herpetiformis: (a) intraepidermal cleavage with acantholytic cells in the upper layers; (b) scanty acantholysis with adjacent eosinophilic spongiosis
Figure 13.3
Pemphigus foliaceus (var.) herpetiformis: (a) direct and (b) indirect immunofluorescence showing intense intercellular IgG deposits within the epidermis
Diagnosis
Pemphigus foliaceus (var. herpetiformis)
Discussion
Pemphigus herpetiformis (PH) is an uncommon intraepidermal autoimmune blistering disease with incidence rates up to 7.3 % among pemphigus patients [15]. This rare variant of pemphigus shows no gender predilection [15, 17, 24], and is predominantly observed in adults [22]. PH exhibits clinical features similar to dermatitis herpetiformis and immunological findings of pemphigus [8]. Since Jablonska et al. first described PH in 1975, nearly 100 cases have been reported [10].
Clinical presentation consists of pruritic vesicles, papules and bullae over erythematous background, arranged in a herpetiform distribution. Some lesions may centrifugally spread, originating annular and polycyclic plaques [22]. Usual sites of involvement are the thorax, torso, and proximal limbs; mucous membranes are usually spared [19, 22]. Differential diagnosis include pemphigus foliaceus, pemphigus vulgaris, bullous pemphigoid, linear IgA bullous dermatosis and dermatitis herpetiformis [6].
Similar to its polymorphous clinical features, histopathologic findings are variable [22], showing spongiosis with eosinophils and/or neutrophils, microabscesses and blister formation, with mild or no evident acantholysis [8, 10, 22].
Diagnostic criteria for PH include: (1) direct immunofluorescence: IgG and complement intraepidermal intercellular deposits [10, 22, 24]; (2) indirect immunofluorescence: circulating IgG antibodies against desmosome components [10, 22, 24]; (3) enzyme-linked immunosorbent assay: anti-desmoglein 1 circulating antibodies (also consider anti-desmoglein 3 and anti-desmocollin 3) [10, 11, 22].
PH pathogenesis remains unclear. Santi et al. reported seven cases of PH in which two patients developed lesions before pemphigus foliaceus (n = 1) and pemphigus vulgaris (n = 1) diagnosis, and five patients who presented lesions consistent with PH during PF (n = 4) and PV treatment (n = 1). Therefore, PH could be a transient, clinical presentation of classical pemphigus [24].
Current evidence suggests the occurrence of an epitope-spreading phenomenon: autoantibodies anti-desmoglein 1 and 3 bind to different antigen sites. Kubo et al. proposed that in pemphigus foliaceus and pemphigus vulgaris, pathogenic IgG autoantibodies disrupt adhesive properties of desmogleins and activate proteinases signaling and release, causing acantholysis. Meanwhile, acantholysis is rarely observed in PH because keratinocyte adhesion mediated by desmogleins is preserved [12]. O’Toole et al. demonstrated that in PH patients, IgG autoantibodies upregulate IL-8 production by keratinocytes, which attracts neutrophils [20]. After recruitment and activation mediated by the Fc portion of IgG, neutrophils secrete proteases leading to spongiosis [10].
IgG subclasses might be another determinant of disease profile. IgG1 and IgG3 are predominant during remission or preclinical asympthomatic pemphigus vulgaris, while IgG4 is a marker of disease activity [2, 25]. Nevertheless, in PH, IgG1 and IgG3, but not IgG4 are able to induce eosinophilic activation and degranulation with release of mediators that promote spongiosis and possibly mild acantholysis [9].
Since neutrophils and eosinophils play an important role in the pathogenesis of PH, dapsone is the first line treatment. Sulphonamide reduces polymorphonuclear chemotaxis, and inhibits tissue damage mediated by lysosomal enzymes and toxic oxygen species [3, 7]. Dosages vary from 100 to 300 mg/day in monotherapy or combined with low dose systemic corticosteroid [1].
PH has a good prognosis with rapid response to therapy in about two thirds of the patients [14], especially when antibody serum titers are low or absent, and eosinophilic spongiosis is observed [1, 5]. As patients with PH may progress to PF or PV, systemic corticosteroid and immunosuppressants should be considered in their treatment [24]. Some cases of PH associated with psoriasis [18, 23], infections [4], neoplasms [13, 16, 19, 21] and drugs [26, 27] were reported, but due to the rarity of this pemphigus variant, a true correlation remains uncertain.
Key Points
Pemphigus herpetiformis is a rare pemphigus variant, with clinical features resembling dermatitis herpetiformis and immunological profile consistent with pemphigusRelated posts:
 An Elderly Patient with a Generalized Pruritic Eruption
A Healthy African Child with Blisters
An Elderly Patient with a Generalized Pruritic Eruption
A Healthy African Child with Blisters
 A 52 Year Old Man with Cerebriform Vegetating Masses on the Scalp
A 52 Year Old Man with Cerebriform Vegetating Masses on the Scalp
 Single Step Multivariant Analysis of Serum Autoantibodies in Autoimmune Blistering Diseases Using BIOCHIP® Mosaic Technology
Single Step Multivariant Analysis of Serum Autoantibodies in Autoimmune Blistering Diseases Using BIOCHIP® Mosaic Technology
 A Chronically Ill Teenager with Blisters and Scars
A Chronically Ill Teenager with Blisters and Scars
 A Man with a Blistering Rash
A Man with a Blistering Rash

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


