Summary
Contour abnormalities in pedicle flap reconstruction are common and easily managed with appropriate revision.
Edema and soft-tissue contour abnormalities present at the time of flap division and inset will not resolve predictably. It is safer to wait until it resolves spontaneously or the flap is converted to a three-stage flap.
After 6 weeks, most pedicle flaps can be aggressively re-elevated and defatted over 80% of their volume.
25.1 Introduction
Over 90% of reconstruction patients would like some improvement of their operative scars and it is incumbent on the treating surgeon to help the patient set expectations and select efficacious and appropriate treatment modalities. 5
Scar massage, silicone sheeting, dermabrasion, pulsed-dye laser treatment, and fat injection have all shown benefit in improving final scar appearance.
25.2 General Principles
Of the two pedicled flaps covered—the nasolabial and the forehead flap—the nasolabial flap is much more likely to suffer partial loss due to its random arterial inflow. Fortunately, even the more tenuous nasolabial flap rarely suffers a complete loss requiring a repeat flap procedure. Usually, the nasolabial flap will suffer only a partial loss that allows sufficient deep soft tissue to develop in the base and allow full-thickness skin grafting as a conversion to a completed reconstruction. Given the geometry of the nasolabial flap design, there is rarely enough length available to salvage the flap-by-flap elevation and re-advancement.
25.2.1 Early Healing Stage
The majority of forehead flap complications in the early healing stage are due to improper flap design, usually as conversion to a random-pattern flap versus remaining axial pattern. Remaining as an axial pattern flap, the forehead flap is very robust and will tolerate significant thinning on inset without distal tip loss. A significant number of well-designed and robust forehead flaps will show early venous stasis reflected in a dusky appearance. This worrisome initial appearance will usually resolve within 24 hours and topical application of nitropaste does speed resolution. 1 For forehead flaps that do in fact progress to partial necrosis, usually manifested by distal tip loss, the reconstruction can be salvaged by simple flap revelation and advancement. 2, 3, 4
25.2.2 Contour Abnormalities and Late Healing Stage Revisions
For nasolabial flaps that heal with significant pincushioning almost all can be managed with significant (>60%) flap re-elevation, aggressive thinning, and re-inset as early as 6 weeks after division and inset. The volume and geometry of nasolabial flaps do not usually tolerate internal or external tacking sutures on inset.
For forehead flaps that present with significant pincushioning or contour abnormalities prior to division and inset, any forehead flap can be converted to a three-stage flap by leaving the flap pedicle intact and flap revelation and inset, including tacking sutures to improve contour. 2, 3, 4 The likelihood of a flap that is significantly thickened or pincushioned before division and inset correctly recontouring after division and inset is very low. The safest and the most time-effective route to achieving acceptable contour is conversion to a three-stage flap with aggressive thinking, tacking suture placement, and re-contouring done at the second stage. The third and final stage, which includes pedicle division and inset, occurs 4 to 6 weeks after the second stage, provided acceptable contour is reached. 4
For forehead flaps that pincushion after division and inset most frequently with disruption or effacement of the alar groove, revision involves direct incision of the alar groove based on the normal contralateral side with careful debulking above the groove and tacking sutures placed during re-insert to maintain the shape. If there is a combined cheek and alar defect, then the same principles can be applied to the cheek–nose junction with direct linear incision along the junction, debulking of the cheek and nasal sidewall, and inset.
Often, patient issues after a successful nasal reconstruction with a forehead flap involve the donor site and not the nasal reconstruction. Frequently, the inset flap pedicle itself can become thickened and distort the eyebrow and if a widened (>1.5 cm) pedicle was required, then forehead scar depression may result.
To address these issues, maximal improvement with nonoperative management, including silicone sheeting, triamcinolone injection, laser therapy, and dermabrasion, is performed. 5, 6, 7 At 4 to 9 months after division and inset, the patient can be returned to the operating room for final revision of the forehead flap donor site scar.
The flap pedicle is re-elevated and maximally thinned before re-insetting or if the geometry of the eyebrow permits is simply excised and the remaining defect closed as a linear incision.
Careful attention is paid to maintaining eyebrow symmetry and position.
If the forehead scar is significantly depressed, the scar itself is bluntly freed from the often adherent skull by elevation from the eyebrow incision with a Penfield no. 4 elevator.
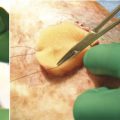
At this point, autologous fat is often injected in a crosshatch pattern with a 21-gauge needle (▶ Fig. 25.1, ▶ Fig. 25.2, ▶ Fig. 25.3, ▶ Fig. 25.4, ▶ Fig. 25.5, ▶ Fig. 25.6).
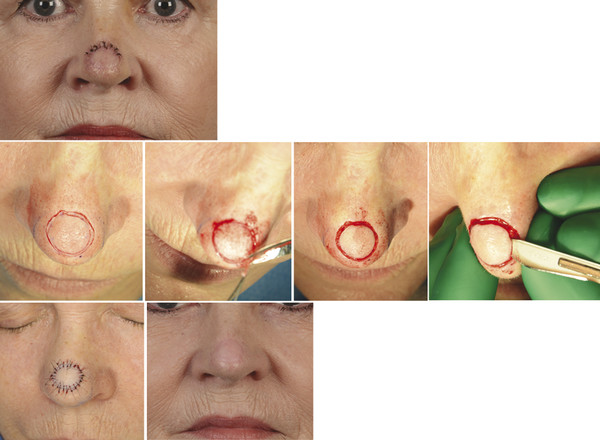
Fig. 25.1 A 66-year-old female status post forehead flap reconstruction of a nasal tip defect. She complained of “bottle-cap” appearance and would have benefited from a subunit as opposed to defect-only reconstruction. Revision performed at 2 months illustrates the ability to fully re-elevate the flap 360 degrees across the perimeter, leaving only a central portion unelevated. Re-inset in this fashion greatly improves flap contour. Final postoperative results shown at 3 months.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


