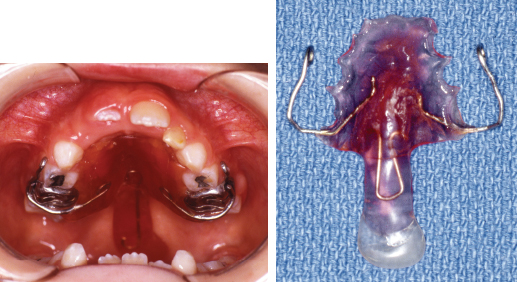
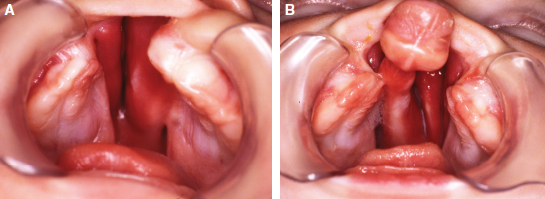
62 ○ Dental management of patients with cleft lip and palate is a coordinated effort among pediatric dentists, orthodontists, oral surgeons, and prosthodontists. ○ Pediatric dental care begins in infancy and continues through adolescence. Although most infants with a cleft are seen soon after birth, the American Academy of Pediatric Dentistry recommends that infants be seen at least after the first tooth comes in or before 1 year of age. ○ Initial management centers on the use of maxillary appliances to assist in the normalization of the cleft defect. ○ The effort in the primary dentition stage of infants with a cleft is to provide preventive and therapeutic oral health care. ○ During the mixed dentition stage, the pediatric dentist assists the orthodontist in providing crossbite correction for the cleft deformity in preparation for alveolar bone grafting by the plastic surgeon. ○ The pediatric dentist and orthodontist work closely during full-banded orthodontic therapy in the teen years to provide the best outcome. Regular dental recall examinations combined with good oral hygiene and preventive practices are necessary for optimal results. Current management protocols have been developed by cleft and craniofacial teams of health care providers from many disciplines. Team care should be based on a philosophy developed by team members and guided by the principles of the American Cleft Palate-Craniofacial Association.1 Team members comprise the medical specialties (plastic surgery, otolaryngology, and pediatrics), the dental specialties (oral surgery, orthodontics, pediatric dentistry, and prosthodontics), and the allied health professionals (audiology, speech pathology, nursing, psychology, and social work). With the more complex cleft and craniofacial syndromic diagnoses, additional specialties are necessary, such as anesthesiology, genetics, ophthalmology, neurosurgery, and radiology. The pediatric dentist is unique among the many team providers involved in caring for patients with a cleft because of the scope of practice. Pediatric dental care begins in infancy with the Infant Oral Health Care Program and continues through adolescence.2 The routine periodicity of dental visits provides an unparalleled opportunity for cleft patients and their dental treatment to be monitored longitudinally.3 Whereas all other cleft team care providers examine and provide services to cleft patients at certain intervals (orthodontists), episodically (oral surgeons), interventionally (speech pathologists), and surgically (plastic surgeons), the pediatric dentist evaluates and observes the developing dentition and monitors overall oral health at 6-month intervals from infancy through adolescence. Among the services provided by the pediatric dentist are preventive dental care, which begins early with the establishment of the “dental home,” caries risk assessment, restorative dental services, space management, nutritional counseling, and trauma management.4,5 This chapter explains the insight and rationale for pediatric dental intervention during the course of cleft lip and palate care. Principles of the American Cleft Palate-Craniofacial Association have been incorporated into an endorsement by the American Academy of Pediatric Dentistry for care of cleft lip and palate patients.6 This dental care is a continuum with similar needs of preventive and restorative dentistry as are required in healthy patients, but with unique procedures and collaboration with specialists for cleft lip and palate management. The location of specific services also may be unique in that many dental procedures are performed in a hospital in conjunction with other specialists on the team. In general, the timing of dental intervention in the cleft habilitation process is correlated to odontogenic and orofacial development. Four classic stages related to the patient’s age have been established that roughly correspond to tooth eruption time and to the establishment of the occlusion.7 The dental cleft team members—oral surgeons, orthodontists, pediatric dentists, and prosthodontists—perform specialty procedures on infants, children, and adolescents with clefts based on dental maturity, age, and behavior and cooperation in coordination with other care providers. Usually, interventions proceed in a specific order, with defined treatment objectives and a timetable for completion. That is not to say, however, that planned, sequential intervention cannot be adjusted. For example, maxillary expansion in the early mixed dentition is normally performed before bone grafting. If the eruption of the maxillary permanent first molars is delayed, it may be necessary to postpone this procedure, because these teeth are necessary for placement of the expansion appliance. Likewise, if the patient is uncooperative for this early phase of orthodontic therapy, the orthodontist may elect to defer treatment until the patient is more mature. Initial cleft management in stage I begins with addressing the immediate issue of infant nutrition and feeding. Because of the nature of the clefting process, infants with either unilateral cleft lip and palate (Fig. 62-1, A) or bilateral cleft lip and palate (Fig. 62-1, B) have unique feeding issues. Adequate nutrition is of utmost importance. The team clinical nurse specialist or the feeding specialist instructs parents in the methods of feeding an infant with a cleft. Various types of infant cleft nipples and techniques have been advocated.8 These were discussed in detail in previous chapters. Most of the time, adequate infant nutrition can be achieved through assisted feeding with a compressible or squeezable bottle or other specialized feeding device.9 In a few special instances (such as in syndromic infants or those with severe facial clefts), the pediatric dentist may need to fabricate a feeding appliance to assist with oral intake. These appliances are constructed on plaster casts made from impressions of the infant’s maxilla. Usually they are designed to obturate the entire cleft defect and to allow food and liquids to enter the digestive tract properly. Fig. 62-1 Infants with clefts at 4 weeks of age. A, Unilateral cleft lip and palate. B, Bilateral cleft lip and palate. The second major consideration at stage I is the use of maxillary appliances, either active or passive and extraoral or intraoral. The sequencing of appliance usage must be coordinated with the initial lip closure. Depending on team protocols and care provider availability, both orthodontists and pediatric dentists (and sometimes prosthodontists) perform these procedures and coordinate care with the plastic surgeon. Active appliances are designed to provide a force to alter relationships of the hard and soft tissues. Such appliances can be either extraoral (such as a head cap or bonnet with tape and straps applied to a projecting premaxilla) or intraoral (such as an acrylic device with springs). Passive appliances use the forces created by lip adhesion or definitive lip repair to stabilize the posterior maxillary alveolar segments while allowing the anterior cleft segments to rotate or “mold” around an acrylic framework (Fig. 62-2). Fig. 62-2 An alveolar molding appliance in place in an infant with bilateral cleft lip and palate. The timing of appliance usage is related to the intent and outcome. True presurgical maxillary appliances (tape across the premaxilla or nasoalveolar molding appliances) are used before initial cheiloplasty and either adjust alveolar segment position or alter tissue form. Presurgical benefits include the adjustment of the cleft tissues to a more ideal relationship before initial surgery to enhance surgical outcome. Passive appliances (including alveolar molding appliances) use the forces created by either lip adhesion or definitive lip repair to provide a force over time and mold the alveolar segments. These appliances allow controlled anterior alveolar segment rotation and reorientation of the maxillary frenum toward the midsagittal plane while maintaining posterior cleft segment position. Considerable controversy exists among clinicians and researchers regarding the purpose for and short- and long-term outcomes of the use of early infant maxillary appliances. In the past, clinicians used “presurgical appliances,” “presurgical orthodontics,” or “neonate orthopedics” with the intent of reducing the magnitude of the cleft deformity and to help to eliminate the need for extensive orthodontics in the future. Many surgeons noted that successful initial lip surgery was easier to attain, but researchers studying the long-term effect of presurgical orthopedics on the growth of the nasomaxillary complex saw little change with the use of early infant appliances. Currently, interest has been renewed in the use of early cleft appliances to assist in “normalizing” the cleft lip and alar cartilage and providing better soft tissue relationships before initial cleft surgery.10 Most researchers agree that the absence of sufficient evidence either for or against the use of presurgical maxillary appliances is because of small treatment populations in cleft teams, lack of longitudinal studies using randomized clinical trials, the length of time necessary to fully evaluate a particular technique or philosophy of treatment, and variables associated with multicenter studies. The increased patient and care provider time and the increased costs associated with infant cleft appliances and the multiple visits required for adjustment must be considered. More complex cleft procedures tend to be performed in urban cleft centers, where many of the team specialists are located. Many cleft patients and their families must travel long distances for such specific interventions. In addition, the increased financial burden may affect the family’s ability to receive care. As a result, care providers must evaluate the benefits of early cleft appliance usage in relation to this additional time and increased cost. During stage I, the pediatric dentist begins infant oral health care. At the first dental visit, the pediatric dentist examines the oral cavity, notes any abnormalities in the hard or soft tissues, and provides anticipatory guidance to parents regarding dental care. Dietary intake of fluoride and the benefits of fluoride are discussed. The problem of early childhood caries and its relationship to prolonged nursing or bottle-feeding and to the frequency of intake of cariogenic foodstuffs is addressed. Finally, common injuries to the erupting primary teeth are discussed, and instructions are given to the parents regarding handling potential traumatic events. One of the major components of the age 1 dental visit is a review of oral hygiene practices for the infant. Proper toothbrushing and flossing are essential to remove plaque and cariogenic bacteria from tooth surfaces. Instruction for parents by the pediatric dental team begins as soon as the first incisors erupt. Using a moistened cloth or gauze square, the parent or caregiver wipes each tooth surface, including those in the cleft area, daily either while holding the child or with the child lying down. Soon after the first primary molars erupt, the parents should begin brushing the teeth using a soft-bristled infant toothbrush. For children younger than 2 years who are considered at moderate to high risk of caries, a smear of fluoride toothpaste should be used. In all children aged 2 to 5 years, a pea-sized amount should be used. Parents and caregivers should be aware of the risks and benefits of fluoride use at an early age in preventing early childhood caries.11 Parents may begin flossing when the gaps between the teeth begin to close. At this stage, the pediatric dentist begins to answer some of the many questions parents have regarding the cleft deformity. These concerns relate in part to congenitally missing teeth in the cleft area, timing of orthodontics, bone grafting, and replacement of missing teeth in primary school-age children and in the teen years. The pediatric dentist should reassure the parents that all of their questions and concerns are priorities in team care and, as a member of the team, explains the procedures and treatment benchmarks at each stage. In some instances, the team members will not only be the diagnostic and treatment planning group but also the providers of the cleft care. In other instances, the team will direct the overall care and provide some of the more complex services with more routine services provided by local care providers. In all cases, the cleft team will monitor the progress of individual services through regular team visits and make appropriate recommendations for subsequent interventions. The primary dentition stage is marked by the complete eruption of all primary teeth and continues until the beginning of mixed dentition with the eruption of the mandibular permanent incisors and permanent molars. The process of tooth eruption in the primary dentition normally begins in the mandibular arch with the eruption of the central incisors at 8 months of age (6 to 10 months 6 1 SD) and in the maxillary arch with the eruption of the central incisors at 10 months of age (8 to 12 months 6 1 SD).12 The normal sequence of primary tooth eruption in both the maxilla and the mandible begins with the central incisors followed by the lateral incisors, first molars, canines, and second molars. In infants and children with cleft lip and palate, eruption of the primary teeth is delayed on the cleft side in both the maxilla and mandible when compared with the homologues on the noncleft side. This delay is statistically significant for the maxillary lateral incisor, the maxillary cuspid, and the mandibular lateral incisor.13 The sequence of primary tooth eruption on the maxillary cleft side is altered, with the lateral incisor erupting last.13,14 The incidence of natal teeth (teeth present at birth) and neonatal teeth (teeth that erupt during the first 30 days after birth) is increased in infants with cleft lip and palate and in the presence of syndromic conditions.15 The major emphasis during stage II is the establishment of the primary occlusion and the promotion of good oral hygiene. Pediatric dental concerns at this time are focused on a good oral health care program at home, prevention of dental caries, restoration of carious teeth, preparation of the teeth for any necessary maxillary appliances, and routine periodic visits to the dental office. During this time, parents and caregivers will continue to have questions regarding the cleft defect and its effect on the primary and permanent teeth. As the primary teeth erupt, parents soon notice that the teeth in the cleft area may appear to be out of position, rotated, tipped into the cleft defect, malformed, discolored, or missing. Many times they may see anterior-posterior malalignment of the dental arches, with the mandible in anterior crossbite. Likewise, they may be aware of a “tipping in” of an alveolar segment, resulting in a posterior malocclusion, and they may become cognizant of supernumerary teeth erupting in or around the cleft site. Some of these issues may be addressed during this stage; others will be deferred until further development of the dentition. The promotion of good oral hygiene that began in infancy is reinforced in stage II as the primary dentition matures. Children with unilateral and bilateral cleft lip and palate have abnormal alveolar segment relationships, with rotation and tipping of the teeth near the cleft defect and in the cleft alveolar segments. Crowding can occur and restrict the ability of the toothbrush to reach difficult areas. In addition, supernumerary teeth, missing teeth, abnormal tooth morphology and hypoplastic enamel, a severely protruding maxilla, and other issues may affect the ability to properly brush and remove bacteria and plaque from the tooth surfaces. These factors put children with clefts at higher risk for the development of caries compared with the general population and require a personalized program of preventive dental care. Streptococcus mutans, one of the most virulent of the caries-producing microorganisms, begins to colonize in the oral cavity around 15.7 months of age, and by the age of 24 months, 84% of children harbor the bacteria.16 In one study, positive cultures of S. mutans appeared at the mean age of 15.3 months, with a positive correlation between the time of acquisition of the bacterium and the number of erupted teeth.17 Most likely, the mode of transmission of S. mutans is oral, from the parent (mother) to the infant.16,17 These microorganisms metabolize carbohydrates, and byproducts of this metabolism then reduce the pH of the oral cavity and initiate the process of caries formation. Most experts agree that the earlier the transmission, the more likely the infant will be at risk for caries. Researchers have long documented that children with cleft lip and palate have a higher incidence of dental caries.18–20 Recent studies have confirmed this observation.21 However, researchers have also noted that there are no differences in the proportion of caries-producing microorganisms at the cleft site when compared with unaffected sites.22 This would seem to indicate that there would not be more carious activity than normal at cleft sites, but conventional wisdom notes that teeth tipped into the cleft area and supernumerary teeth that are present there collect plaque and commonly become carious. In general, any caries risk factor that may contribute to the caries process in typical infants and children may also be applied to special patients, such as those with cleft lip and palate. Some of these factors are previous caries, salivary disease, the presence of orthodontic appliances, between-meal sugar exposure, intake of carbonated beverages, inadequate fluoride exposure, poor toothbrushing habits, and lack of regular dental visits. In addition, certain factors may contribute to the apparent increase in dental caries in infants and children with clefts specifically, such as the position of the teeth in the dental arch, crowding of teeth in the cleft area, difficulty in brushing in the altered alveolar segments, and oral hygiene and dietary habits. Recently researchers have developed new strategies for the prevention of caries in patients with cleft lip and palate that can assist cleft teams in developing oral health care programs for their patients.23 Maxillary appliances may be indicated in the primary dentition stage to assist specialty providers in the course of cleft habilitation. In selected patients, for example, obturators or palatal lift prostheses may be used to manage velopharyngeal dysfunction (Fig. 62-3). In other patients, appliances may be used to obdurate oronasal fistulas. The pediatric dentist or the prosthodontist will use a stone cast made from an impression of the cleft maxilla to construct these palatal appliances. Wire clasps for retention are placed posteriorly to surround the molar tooth and hold the appliance in place.
Pediatric Dentistry for the Cleft-Affected Patient
Donald V. Huebener
KEY POINTS
SEQUENCING OF DENTAL CARE IN CLEFT PATIENTS
Stage I: Initial Management and Maxillary Appliance Stage, Birth to 24 Months

Stage II: Primary Dentition Stage, 2.5 to 6 Years of Age
Oral Hygiene for Children With Clefts
Cleft Lip and Palate and Dental Caries
Maxillary Appliances
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine