(1)
Yotsuya Medical Cube, Chiyoda-ku, Tokyo, Japan
Basic Principles
Cases involving reconstruction of the knee include an open fracture with tissue loss over a wide area, osteomyelitis cases, and cases of reconstruction after resection of a malignant tumor. All of these cases require a flap with significant volume, so muscle flaps or musculocutaneous flaps are selected.
For muscle flaps using reconstruction material from the lower leg, despite considerable operative stress, there is only a small transfer distance, so free tissue transfer is often the selected option. Severing the muscle ends and creating a complete island flap increases the transfer distance of the muscle flap, enabling it to become the first option. Free tissue transfer is indicated for cases with losses exceeding the size of the lower leg muscles, however in such cases, the popliteal fossa region can be used for an anastomotic vessel based on the Godina Method.
Selectable Flaps and Surgical Procedures
Gastrocnemius muscle flapFree latissimus dorsi musculocutaneous flapSaphenous flapSuperior medial knee flapSuperior lateral knee flapThe difficulty level of each surgical procedure is shown subsequent to the procedure title (e.g., Level of Difficulty: 2). The levels range from 1 to 5, with level 1 indicating a preliminary level and level 5 indicating a very advanced level.

14.1 Gastrocnemius Muscle Flap (Level of Difficulty: 3)
Information
Vascular pedicle Sural artery
Size Size of the medial or lateral head of gastrocnemius (excluding Achilles tendon)
Advantage Can obtain sufficient thickness for the muscle flap. Has stable vascularization. Can obtain muscle flap in the same operating area
Disadvantage Requires skin graft
14.1.1 Operation Procedures

Fig. 14.1
Procedure 1: An incision is made to the center of the lower leg and the boundary of the medial and lateral head of gastrocnemius confirmed
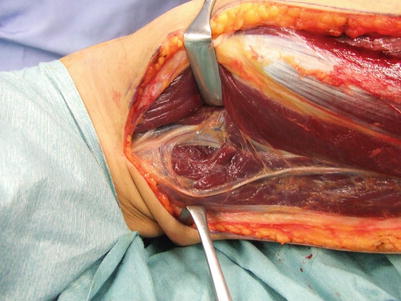
Fig. 14.2
Procedure 2: The sural artery that emerges from the popliteal artery at the proximal gastrocnemius muscle is confirmed as entering the medial and lateral head of gastrocnemius
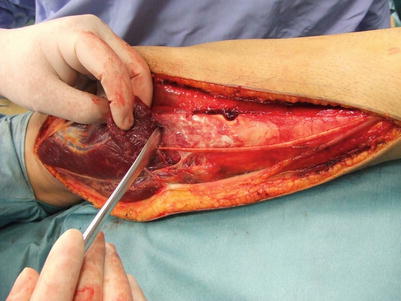
Fig. 14.3
Procedure 3: Either the medial or lateral head is selected, and the muscle is detached from the Achilles tendon
Note
Photo shows removal of lateral head of gastrocnemius of right lower leg.
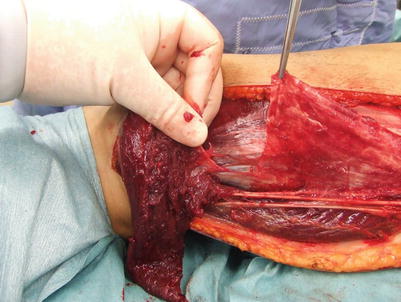
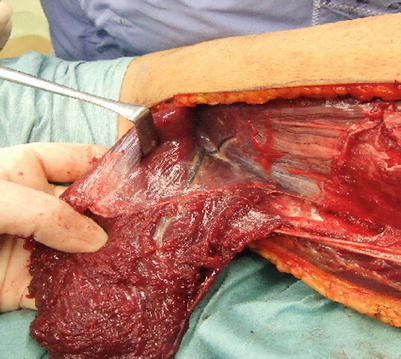
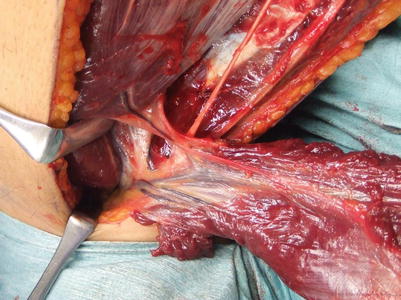
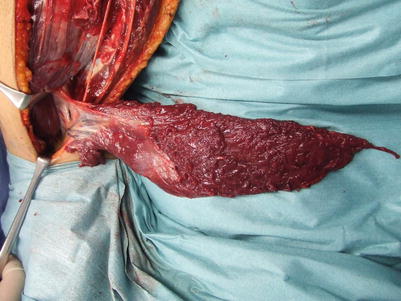
Fig. 14.4
Procedure 4: The separated Achilles tendon is left as it is
Fig. 14.5
Procedure 5: The muscle is detached moving towards the proximal end
Fig. 14.6
Procedure 6: While confirming the sural artery, other branches are ligated and cut, and the proximal gastrocnemius muscle is severed
Fig. 14.7
Procedure 7: The muscle flap is elevated as a complete muscle island flap with the vascular pedicle only
Note
If the proximal end of the muscle is not fully cut here, then it won’t be possible to obtain sufficient mobility.

Fig. 14.8
Procedure 8: Case: Anterior cruciate ligament rupture case with tibia fracture and skin defect of patella region










