(1)
Yotsuya Medical Cube, Chiyoda-ku, Tokyo, Japan
Basic Principles
The plantar MP joint is a weight bearing area, and a thick tissue is required for reconstruction. However, taking into consideration comfort when walking, there are limited options when selecting skin flaps based on tissue characteristics and thickness.
It is not necessary to pro-actively pursue a sensory reconstruction, but if a similar tissue is used for reconstruction, it is easier to obtain protective sensation.
For reconstruction of the plantar forefoot, in principle, plantar flap transfer from the unaffected foot is not an option.
First option: Distal transfer of medial plantar flap from affected side. In order to increase the transfer distance, if the vascular pedicle is detached from the tarsal tunnel and transferred forward, it is possible to reconstruct a more distal area.
Free flap:
– Small defect
• Abdominal perforator (DIEP) flap
• Combination with medial plantar island flap
– Large defect
• Bi-lobed scapular flap
• Latissimus dorsi muscle flap + skin graft
• Anterolateral thigh flap
Selectable Flaps and Surgical Procedures
Medial Plantar FlapFree abdominal perforator flapFree scapular flap (Bi-lobed scapular flap)Extensor digitorum brevis muscle flapAnterolateral thigh flapThe difficulty level of each surgical procedure is shown subsequent to the procedure title (e.g., Level of Difficulty: 2). The levels range from 1 to 5, with level 1 indicating a preliminary level and level 5 indicating a very advanced level.

19.1 Bi-lobed Scapular Flap (Level of Difficulty: 4)
Information
Vascular pedicle Dissected and harvested from circumflex scapular artery to subscapular artery. Length of vascular pedicle 10 cm and diameter 2 mm
Size The size of a scapular flap that can be sutured closed is around 20 cm long with a width of 8–10 cm, and this can be combined with a flap of longitudinal length 15–20 cm and width 10 cm
Indication For large skin defects
Advantage Has thickness. Technique is simple and has stable blood flow. It is possible to create a large flap
Disadvantage Can require change of body position. Not possible to reconstruct sensory function
19.1.1 Operation Procedures

Fig. 19.1
Procedure 1. Case of necrotic skin on plantar forefoot weight-bearing region

Fig. 19.2
Procedure 2: Patient is placed in the lateral recumbent position. The circumflex scapular artery emerges from almost the center of the acromial process and the inferior angle of the scapula and passes through the scapular triangular space (area in between the teres minor muscle, teres major muscle and long head of triceps brachii muscle), emerging subcutaneously. Therefore, this area must be included in the skin flap design
Note
In order to create a bi-lobed flap, an additional skin flap is added running longitudinally along the lateral border of the scapula.
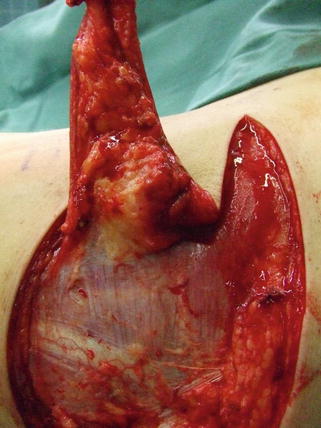
Fig. 19.3
Procedure 3: An incision is made in the distal margin of the skin flap, and the skin flap is detached moving from the medial side of the back to the lateral side
Note
The individual fascia of the back muscles such as the infraspinatus muscle and the rhomboid major muscle are left as is, and the skin flap is elevated with the hazy fascia tissue above that included.
When the skin flap is turned over and detached close to the scapular triangular space, it is possible to confirm the vascular pedicle through the thin fascia. Blood vessels comprise both an ascending branch and a descending branch, so an incision is also made in the lateral border of the scapula and detachment conducted.
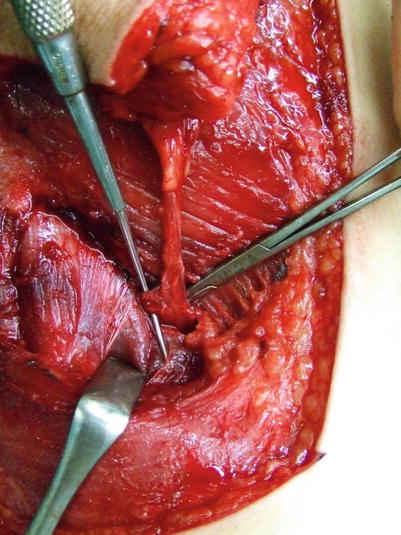
Fig. 19.4
Procedure 4: Confirming the path of the vascular pedicle, it is dissected from above the individual fascia of the infraspinatus muscle, teres major muscle and teres minor muscle, securing the stem of the circumflex scapular artery, with dissection continued inside the scapular triangle
Note
Even if it is not possible to confirm/detach the vascular pedicle of the parascapular flap, if the flap was harvested as a fascia flap along the lateral border of the scapula then it will have been automatically included. If wanting to include part of the scapula, confirmation is made of the descending branch of the circumflex scapular artery, and the lateral border of the scapula is harvested with the teres minor muscle attached.