CHAPTER 20 Hair Restoration in Men
Summary
Hair restoration in men is an important component of aesthetic surgery, and with the newer techniques of follicular unit extraction (FUE), it is more readily within the practice scope of plastic surgeons. In addition to hair transplantation to the scalp for male pattern hair loss, hair restoration incorporates the skills of diagnosis and medical therapies, as well as surgical therapies. Other procedures include eyebrow and beard restoration, and the one-stage hairline- lowering surgery.
Introduction
Over the past 60 plus years, hair restoration surgery has become one of the most popular aesthetic surgery procedures performed on men. Development in techniques, expansion of applications, and a rise in the public awareness have been the driving forces in the growth of hair-restoration surgery. Today, results are truly undetectable—even with one’s hair shaved—leading more men than ever to regain follicles and confidence by having not only fuller heads of hair but also thicker beards, more prominent eyebrows, and correction of less aesthetic “pluggy” appearances and potentially visible wide donor site scars to more natural-appearing results.
As described by Orentreich in the 1950s, who was not privy to the more microwork done by the Japanese 20 years earlier for eyebrow and pubic hair restoration, 4-mm sized grafts containing eight to as many as 20 hairs apiece were the foundation for hair transplant procedures. While one could see some benefit to “pluggy” hair over no hair, the evolution proceeded to smaller 2-mm plug grafts to eventually, in the 1980s and 1990s, micrografts (one and two hairs) and minigrafts (three to six hairs).
It was not until follicular unit grafting (FUG) in the late 1990s became the standard of care that hair transplant results could consistently be natural in appearance when performed properly, as each graft consists of a follicular unit, which is the natural occurring bundling of one to three, sometimes four hairs, as they grow in the scalp. Through dissection of a donor strip under the microscope, each FUG is free from all surrounding nonessential skin and can be transplanted into small recipient sites, typically 0.5- to 0.8 mm in size.
The final evolution in hair restoration has been FUE. A new and improved version of the old “plug” grafts obtained using 3- and 4-mm-sized punches, FUE grafts are also obtained one at a time but using much smaller, typically 0.8- to 1 mm, punches. Like FUG, each FUE graft contains a single follicular unit of typically one to four hairs and is capable of creating truly natural-appearing results when transplanted properly into the areas of hair loss, but with one major advantage: FUE avoids altogether a linear donor site incision scar, instead these punch holes are allowed to heal up secondarily leaving minimally if at all detectable tiny dots.
As these more modern FUE and FUG techniques are able to transplant hairs as they grow naturally in the scalp, three notable developments have occurred in the specialty. First, two other techniques to treat hair loss—scalp reduction surgery and scalp flap surgery—are now obsolete as they are unable to achieve the same degree of naturalness and incur potentially significant scarring. The exception to a surgical technique no longer having applicability is the hairline-lowering or forehead reduction surgery, also called the surgical hairline advancement, that in the appropriate patient is unsurpassed in its ability to bring forward the entire hairline via a trichophytic hairline incision. The second development is the extension of hair restoration for a variety of nonscalp applications, including eyebrow, beard, and chest hair restoration. The third and final development is the expansion of hair restoration into the armamentarium of many plastic surgeons, as an FUE procedure can be performed with just one or two trained hair technicians assisting the surgeon, instead of the larger team required to perform the meticulous dissection of FUG. At the time of the writing of this chapter, robotic devices for FUE graft extraction have an inconsistent application, and their tool for recipient site creation is less reality than concept. However, further developments in capabilities should potentially at some point in the future make them comparable and maybe even superior to human-guided motorized drills for graft extraction and a surgeon making each recipient site one at a time by hand.
Physical Evaluation
Close examination of the areas of male pattern baldness (MPB) of the scalp includes the following:
Degree of hairline recession.
Degree of miniaturization versus actual loss of hairs—an important distinction because a thinning appearance caused by diffuse miniaturization is more challenging to treat with transplants.
Degree of hair loss of the crown next to the frontal portion is the most common to undergo hair loss in MPB and can be more challenging to treat with transplants.
Degree of hair loss of the midscalp and temporal regions including the lateral temporal horns and the temporal points that predict progression to a more advanced degree of hair loss.
Color of the scalp, where a light scalp with dark hair shows more of the thinning, and makes for less impressive hair transplant results.
Close examination of the potential donor areas (sides and back of the scalp) to predict total number of grafts available for eventual transplantation. This includes an assessment of the density of the hairs, the number of hairs per follicular unit (ideally the majority will have two and three hairs so as to create more density), the total size of this donor area with an eye toward predicting how much of this area will be decreased in size with progression of MPB (discussed later).
Examination globally of the shape and proportions of the face and forehead to guide hairline design.
General physical health including age.
When a nonscalp hair transplant is the desired procedure, the degree and pattern of hair loss of the eyebrows, beard, and/or chest.
When hairline-lowering surgery is considered to reduce an overly high forehead, an assessment of scalp laxity of which a moderate amount is required to achieve nice results.
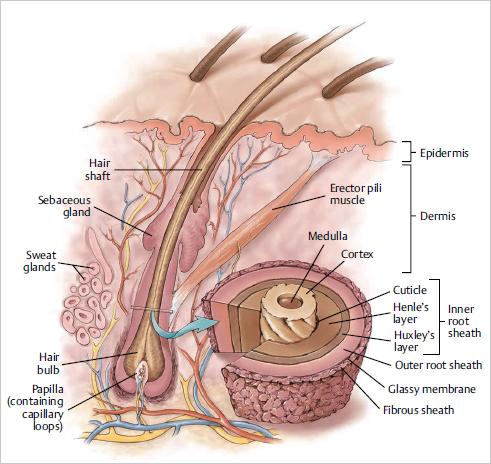
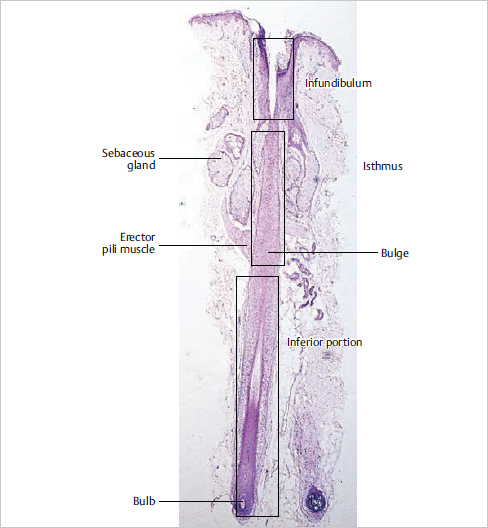
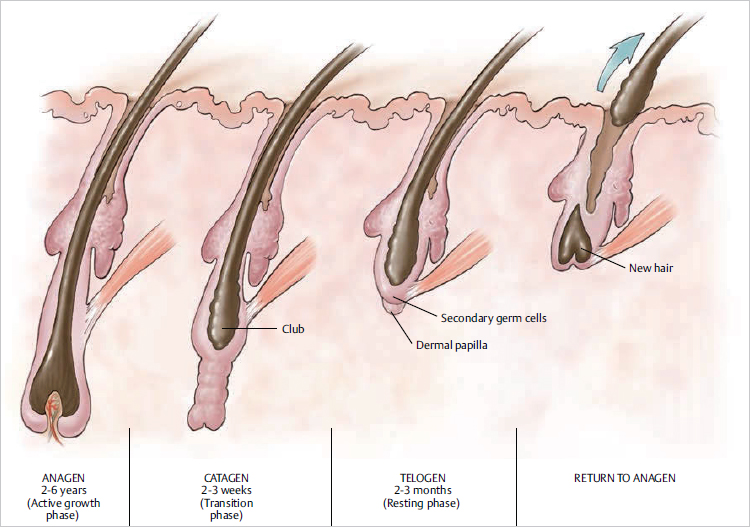
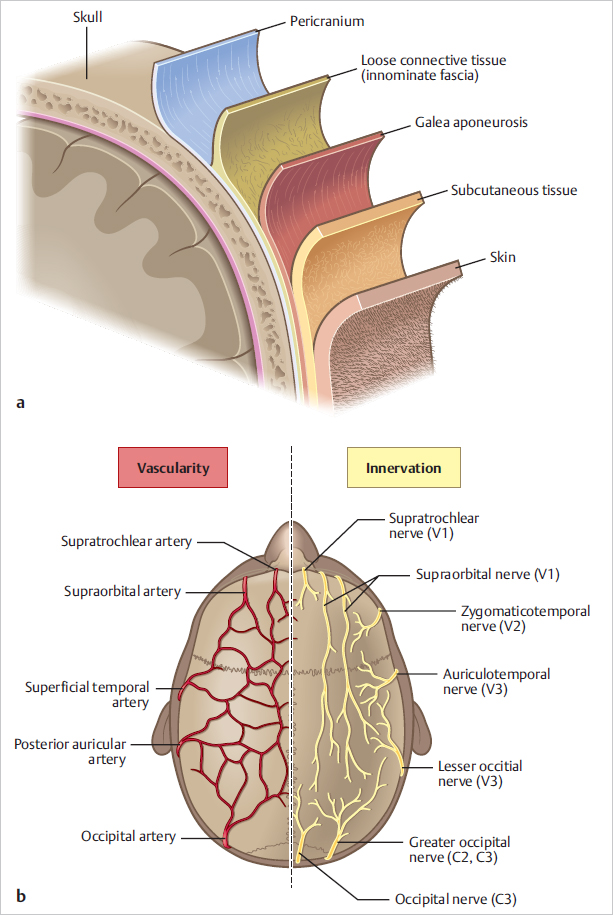
Anatomy
Fig. 20.1 , Fig. 20.2 , Fig. 20.3 , and Fig. 20.4 are relevant to the art of hair restoration.
Patient Selection
Besides the requirement for the patient to be medically able to undergo an elective surgery that entails the making of typically thousands of tiny recipient site incisions and donor site extractions (FUE) or a donor site incision (FUG), the most important part of patient selection is making sure he has realistic expectations and understands the progression of MPB. Hair transplantation is not a “cure” rather a treatment to address the current degree of hair loss that takes proper consideration of the almost sure progression of hair loss that continues throughout nearly every male patient’s lifetime. The 32-yearold man with crown hair loss, or the 24-year-old man with early frontal thinning, for example, must realize that he will progress to a more advanced degree of hair loss, and therefore hair restoration is likely not the best option at this time, instead relying on medical therapies for the possibility of the prevention of further progression. Pity the young patient who gets treated by a surgeon who disregards (or is ignorant) of this fact and receives a hairline that will soon be too low to look natural or has relatively too many grafts extracted and runs out of donor hair to keep up with progressive hair loss. Without overstating the obvious mantra of surgeons, knowing on whom not to operate is more important than knowing how to operate, which is especially relevant in treating MPB. Not to imply that young men should never undergo a hair transplant—rather the realistic surgical approach is to create a conservative restoration, including a hairline that will appear natural not only with increasing age but with progressive hair loss, and that accounts for the fact that with progression of hair loss the demand for hairs increases while the supply of donor hairs decreases ( Fig. 20.5 ).
The presence of hair miniaturization in an area to potentially be transplanted can be a challenge. This miniaturization is part of the natural progression of hair loss, created by a higher ratio of vellus to terminal hairs, which is a step toward the absence of hair in an area. Miniaturized hairs are more susceptible to shock loss, or to falling out when a hair transplant is performed. This shedding may be caused by a variety of phenomena—swelling, a reaction to anesthetics, or the mechanical direct trauma to their follicles by the making of recipient sites. To minimize the incidence of shedding, several steps can be taken:
Avoid injecting epinephrine into the recipient area.
Use smallest possible recipient sites and carefully make slits.
Use a low volume of anesthetic.
Administer oral steroids.
Two other steps that can help minimize shock loss are as follows:
Administer minoxidil and/or finasteride and/or laser light therapy for at least 4 weeks prior to the procedure.
Simultaneously inject platelet-rich plasma (PRP) with a hair transplant.
Taking all these steps, shedding after a hair transplant can be avoidable in nearly all patients.

Steps for Hair Transplantation
Preoperative Preparation
Routine preprocedure precautions are similar to those of any other elective plastic surgery procedure. As intraoperative bleeding can make graft extraction and planting quite challenging, all anticoagulants including aspirin and vitamin E for 10 days and anti-inflammatories and alcohol for 3 days must be avoided. In addition, vitamins K and C can help with hemostasis and control of swelling. Unless the procedure is to be performed under twilight sedation, the patient may have a regular breakfast.
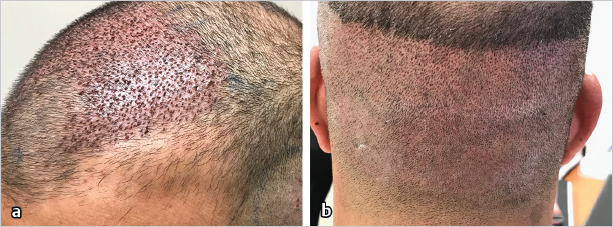
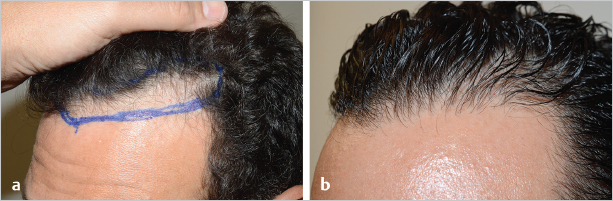
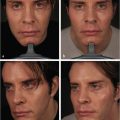
For large FUE cases, most of the back and typically the sides of the head will be shaved down, so the patient is advised that for the first 4 days after the procedure he may not be presentable without a hat ( Fig. 20.6 ). A newer “no-shave” FUE technique avoids the shaving of the head, permitting the patient to be presentable the very next day ( Fig. 20.7 ). With this technique, only one of every three follicular units is shaved so they can be extracted leaving the hairs the normal length. Smaller FUE cases of typically 700 or fewer grafts can obtain the grafts by shaving either the bottom half of the back of the head, so that at 4 days, it appears as if a “fade” haircut was given, or by shaving horizontal tunnels from where grafts can be harvested that can be concealed by the overlying longer hair.
Hairline Design
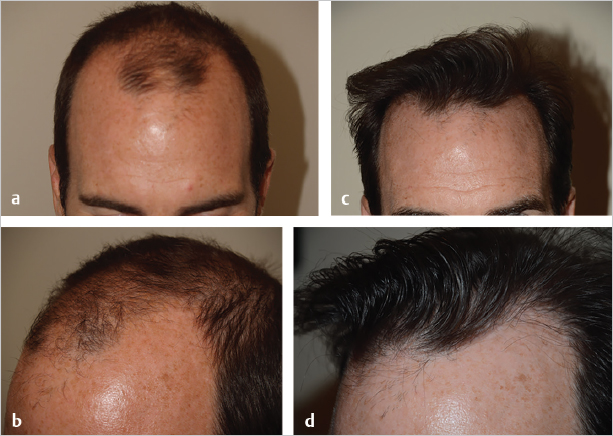
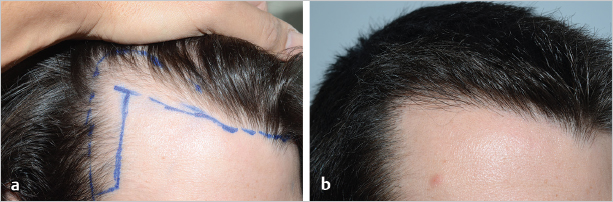
Perhaps no aesthetic step is more important in hair-restoration surgery than the design of the hairline. A large number of factors must be accounted for: patient age, shape of the face, goals, donor supply, existing anticipated future hair, and of course the patient’s gender are the most important. The surgeon can never be faulted for placing the hairline relatively high. A good reference point for the male hairline is to centrally have it start at the junction where the vertical forehead meets the horizontal scalp—a zone typically located 8 to 10 cm above the root of the nose. From this central point, the hairline continues laterally to create frontotemporal recessions that on profile view appear to be at least slightly to moderately receded, avoiding a rounded out or unnatural “simian” appearance ( Fig. 20.8 , Fig. 20.9 ). Note that this is quite different from women in whom rounded hairlines are typically the aesthetic goal.

Other potential components of the scalp that can be restored include the temples or temporal points, the midscalp, and the crown. It is usually best to avoid restoring the temporal points in younger patients, for with future hair loss these temples will only recede further. In the 35-year-old plus patient, conservative temporal filling in can create a more youthful appearance ( Fig. 20.10 ). Like the temples, and for the same reason, crown coverage is best reserved for older patients who are less likely to experience significant future crown hair loss, otherwise as the crown continues to enlarge, more transplants will be required to chase this expanding area, potentially consuming large numbers of grafts. Midscalp coverage is an extension of frontal coverage and in most cases can be safely performed without fear of creating unnatural appearances in the future.
For the hairline-lowering or forehead reduction surgery, the entire frontal-hairline is brought down and forward, keeping relatively the same shape. The scalp’s mobility determines the amount of lowering that can be achieved, usually somewhere between 15 and 25 mm but in cases of excellent scalp mobility as much as 30 mm or more ( Fig. 20.11 ). The anticipated central and frontotemporal points are marked out to serve as landmarks.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


