CHAPTER 19 Adult Otoplasty
Summary
This chapter will cover standard otoplasty (setback only) as well as the combination of setback and reducing the size of the auricle.
Introduction
From a technical point of view, adult otoplasty is one of the simplest procedures in the standard armamentarium of the aesthetic surgeon. Despite the apparent simplicity, however, otoplasty procedures are associated with a relatively high rate of complications and suboptimal results. Male hairstyles more frequently reveal these imperfect results and asymmetries, making otoplasty in men slightly more challenging than in women. Adding to the visibility afforded by traditionally male hairstyles, the adult male cartilage is often stiffer and more prone to undercorrection. Finally, the perceived simplicity of the procedure makes complications and results that fall short of expectation more surprising for many patients and adds to the frustration.
The author has performed otoplasty with regularity for 30 years, and while the surgical results have not been without disappointment, the biggest positive increment in the learning curve came with an appreciation of the surgical end point. It may be utterly obvious, but until the surgeon has a firm grasp of what he or she is aiming at, optimal results can be elusive. As emphasized below, the intraoperative view of the helical contour when viewed from behind provides an almost foolproof method of ensuring good results. The author has preferences regarding techniques, which will be explained later, but undoubtedly there are techniques that produce similar results as long as a harmonious, natural-appearing end point is the goal. The aesthetics matter, not how one gets there.
This chapter will deal with standard otoplasty (setback only) as well as the combination of setback and reducing the size of the auricle.
Physical Examination
The first requirement of the physical examination is determining whether the patient’s ears are just prominent (but otherwise normal in size and shape) or whether, in addition to prominence, there is a significant abnormality of size and/or shape. And of course, there is the occasional patient whose ears are not prominent at all but are, for example, too large and/or abnormally shaped (e.g., Stahl’s ears).
Multiple choice examinations never fail to mention an underdeveloped antihelix and a prominent concha as explanations of auricular prominence. While those characteristics are components of prominent ears, they are not the only issues, and concentration on these two anatomical phenomena to the exclusion of some others is a ticket to disappointment.
There are two things that make the upper third of the auricle prominent, three things that potentially make the middle third prominent, and one thing that makes the lower third prominent.
Causes of Ear Prominence
Upper third: Prominence of the upper third is related not just to the underdevelopment of the antihelix but to the angle that the ascending helix makes with the temporal scalp. As will be discussed below, it is possible to recreate the antihelix and still have a wide angle where the ascending helix leaves the plane of the face and becomes the helical rim.
Middle third: Prominence of the middle third of the auricle is the result of some combination of underdevelopment of the antihelix, height of the concha, and the angle that the concha makes with the occipital scalp.
Lower third: The only phenomenon that causes the lower third of the auricle to appear prominent is an overly protruding lobule. In the author’s opinion, a prominent lobule is unrelated to the tail of the helix and therefore will not be reliably corrected by repositioning the helical tail.
If the patient also has a degree of macro- or microtia or abnormal contour (underdevelopment of the helical rim, etc.), then the analysis and treatment plan must include attention to those issues, not just the prominence. As will be discussed below, it is usually straightforward to make large ears smaller but making small ears larger is usually not practical unless the deformity is significant; reconstructing an auricle from rib cartilage is a significant undertaking. Contour issues such as underdevelopment of the helical rim, Stahl’s ear, question mark ear, etc. may also be addressed at the time of the otoplasty.
Anatomy
Male patients do not differ from female patients with regard to the anatomy of prominence, but the adult male cartilage is often thick and stiff and this anatomical difference affects the treatment to some degree.
The deformity is analyzed, as mentioned above, in terms of thirds. A patient may have one of the “thirds” that is prominent (e.g., only the middle third) or may have prominence of all three “thirds.”
Patient Selection
The identification of patients with prominent ears is usually not a challenge. As mentioned above, the key is determining what part or parts of the ear is/ are prominent. There are patients, however, and they are usually male in this author’s experience, who attach significance to extremely minor auricular prominence, or who are convinced they need an otoplasty when there is no demonstrable abnormality. These patients do not make good surgical candidates any more than a rhinoplasty patient who sees a deformity that the surgeon cannot appreciate.
Steps for Otoplasty
Incision
The standard incision is made in the depth of the retroauricular sulcus ( Fig. 19.1 ). At the caudal aspect, a triangle of skin is frequently removed from the medial surface of the lobule, without compromising the lobular sulcus or the ability to have ear piercing, to facilitate lobule repositioning. At the cranial aspect, the incision is brought out of the sulcus along the medial surface of the antihelix. The incision does not extend closer than 1 cm to the helical rim, because if hypertrophic scarring results, that scar could be visible from the lateral view.

Exposure
The medial surface of the auricular cartilage is exposed, immediately on the surface of the cartilage. Care is taken at the tail of the helix to preserve the connection between this structure and the rest of the cartilage and to preserve the connection between this structure and the lobule. Soft tissue is removed from deep to the concha. Dissection is performed in the depth of the lobular sulcus to expose the concha for later lobule repositioning.
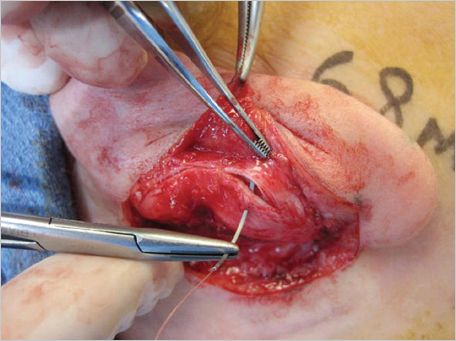
Conchal Resection
In the majority of cases, the middle third of the ear is approached using a combination of conchal resection and conchal setback. A small crescent of cartilage is removed from the junction of the floor and posterior wall of the concha. Usually no more than 3 mm is removed at the central portion of the crescent. Larger resections may cause a visible deformity. The crescentic defect is approximated with clear nylon sutures that are cut immediately on the knot ( Fig. 19.2 ).
Mustarde Sutures
A series of mattress sutures between the scapha and concha and between the scapha and triangular fossa will be placed, but at this point in the procedure only the caudalmost Mustarde sutures are placed beginning at the tail of the helix and extending into the middle third of the auricle. These sutures are placed now, rather than later when the rest of the Mustarde sutures are placed, because the next few maneuvers make visualization of these areas more difficult.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


