CHAPTER 21 Platelet-Rich Plasma and Microneedling in Male Pattern Hair Loss
Summary
Microneedling in conjunction with platelet- rich plasma (PRP) injection to the scalp has been shown to be helpful for stimulating hair growth in men and women with androgenic alopecia, alopecia areata, and discoid lupus. Microneedling the scalp has shown to increase PRP absorption by up to five times versus no microneedling because of the microchannels created in the stratum corneum. This chapter covers evaluation, patient selection, and the steps to take for PRP and microneedling.
Introduction
Platelet-rich plasma (PRP) has been used in cosmetic and maxillofacial surgery since the early 1990s. Surgeons noted faster healing time when PRP was used intraoperatively. Since then, many specialties, including orthopedic and spine surgery, have added PRP to their routine for improved wound and injury healing.
When platelets are separated from whole blood and then concentrated and activated, the growth factors initially promote hemostasis and can decrease inflammatory response. Over time, the platelets can aid in collagen production and increased vascularity. For this reason, microneedling in conjunction with PRP injection to the scalp has been shown to be helpful for stimulating hair growth in men and women with androgenic alopecia, alopecia areata, and discoid lupus. Microneedling the scalp has shown to increase PRP absorption by up to five times versus no microneedling caused by the microchannels created in the stratum corneum.
Physical Evaluation and Patient
Indications
Patients who have been diagnosed with androgenic alopecia, alopecia areata, or discoid lupus and have not had success with other treatments.
Contraindications
Patients with any kind of platelet dysfunction.
Patients with an active infection process of the scalp.
Patients on anticoagulant therapy.
Patients that report allergies to local anesthetics.
Patients with cancer.
Patients should avoid nonsteroidal anti-inflammatory drugs for a minimum of 2 days pre- and postprocedure. Also, note that oral steroid use should be stopped 1 month prior to procedure and smoking or having a recent illness could impair results. Patient should be made aware of all contraindications.
Anatomy
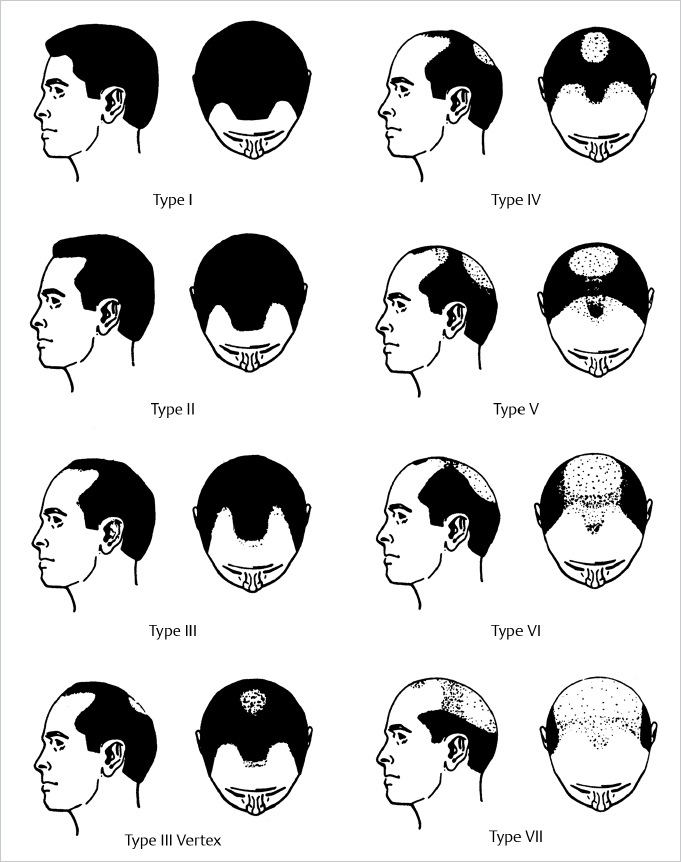
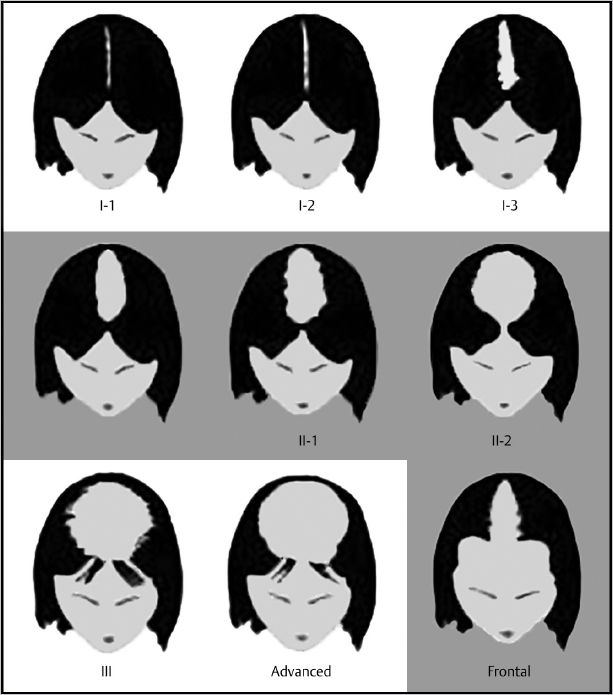
Male pattern baldness begins with a receding hairline and a thinning of the crown. Female pattern hair loss typically begins at the midline of the central scalp and outward. The hairline is usually retained ( Fig. 21.1 , Fig. 21.2 ).
Steps for Platelet-Rich Plasma and Microneedling
This procedure should be performed as a sterile minor procedure. First, create a grid on treatment area in 1 × 1 cm blocks ( Fig. 21.3 ). Do a regional block of the area using 1% lidocaine with epinephrine or a topical anesthetic. Draw six tubes of venous blood into (acid citrate dextrose) ACD A tubes. Place in centrifuge for 2 minutes at 3,400 rpm ( Fig. 21.4 ). Using a sterile 18-gauge spinal needle and 20-cc syringe, draw off the plasma all the way to the buffy coat layer. Evenly distribute the plasma in the syringe into plain red top tubes. Centrifuge for 2 minutes at 3,400 rpm. Gently remove red top tubes from the centrifuge, and you will notice a platelet pellet at the bottom. Using a sterile 18-gauge spinal needle and syringe, draw off the 75% of platelet-poor plasma from the top of tube and discard. Gently aerate the remaining plasma and platelet pellet using the spinal needle and syringe to suspend and distribute the platelets in the remaining plasma of each tube ( Fig. 21.5 ). Draw the PRP from each tube into sterile syringes. The patient can be placed supine or prone based on the practitioner’s comfort or bed type ( Fig. 21.6 ).
Prep treatment area with a Hibiclens solution. Begin microneedling the site following the grid. A 0.75-mm tip is acceptable. Begin with light pressure in a circular motion. Ensure that you see pinpoint bleeding ( Fig. 21.7 ). Draw 1 unit of calcium chloride into several tuberculin (TB) syringes. Calcium chloride is the platelet activator and should not be mixed with PRP until immediate use. Make note of total amount of PRP so that it can be evenly distributed. Fill one of the syringes with PRP and a 25-gauge needle. Inject 0.1 mL in a linear pattern approximately 1 cm apart ( Fig. 21.8 ). Gently massage treated area after PRP injections are complete ( Fig. 21.9 ). Advise patient not to wash hair until the following day.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


