CHAPTER 4 Techniques for Forehead Rejuvenation
Summary
Aging in the upper face can create a tired, unhappy, or even angry appearance. Surgical procedures to rejuvenate the forehead and brow can be very impactful to a person’s overall expression and are thus very rewarding for the patient and surgeon alike. This chapter reviews important features to consider when assessing the aging brow and highlights key differences encountered in the male patient. Various surgical options are presented. Advantages and drawbacks for each approach are described, as are technical points to executing the surgery.
Evaluation of the Aging Forehead and Brow
Facial rejuvenation requires a comprehensive approach to the structures of the face and their interactions. No one feature or area should be considered in isolation, even if patients present with a single area of concern. The contribution of brow ptosis to an aged facial appearance is frequently overlooked but must be considered to achieve a natural, balanced, and aesthetic result.
In evaluating the aging forehead and brow, important features to consider are as follows:
Brow position and shape.
Orbital crowding.
Rhytids.
Skin quality and areas of excess skin.
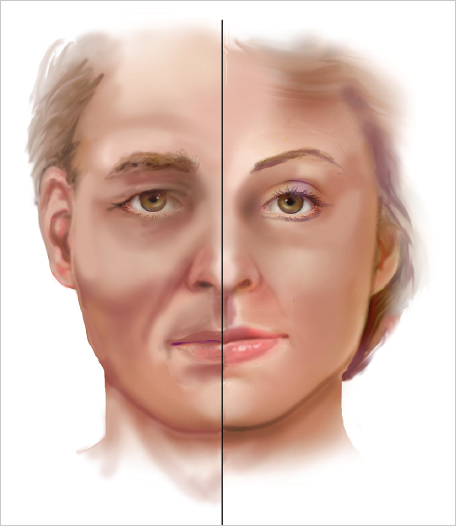
Rejuvenation of the male brow carries distinct challenges in each of these areas, beginning with recognizing key differences in the ideal male brow shape. The male brow overlies the supraorbital rim, typically several millimeters lower than the position observed in women. It has much less of an arch than in females, is generally thicker, and is more prominent laterally ( Fig. 4.1 ). With age, the brow tends to become deflated and ptotic, and can encroach on the lateral upper eyelid creating orbital crowding.
The aesthetics of the brow are influenced by the shape or convexity of the forehead, the position of the hairline, and thus the height of the forehead, as well as the thickness of the retro-orbicularis oculi fat (ROOF). The male forehead is generally more vertical in its contour, and the hairline is more often high or receding. Even when a patient’s hairline is favorable at the time of consultation, it is advantageous to assess its stability so that scars are placed optimally for both current and future hair patterns.
Forehead, glabellar, and lateral orbital rhytids, or crow’s feet, are characteristic of aging in the upper face. These lines are generally deeper in the male patient and more often present at rest. Horizontal forehead lines are more common in men.
Men tend to have thicker, more sebaceous, and less elastic skin, and thus typically form less favorable scars. With fewer recourses to camouflage scars, such as makeup and varied hairstyles, optimizing scar position and scar quality in the male patient is essential.
Skin excess of the upper lid frequently accompanies brow ptosis and often requires blepharoplasty to satisfactorily rejuvenate the periorbital region. Excess skin can also be present over the nasal radix and requires a different approach than the muscle modification used to address glabellar rhytids.
Goals of Forehead Rejuvenation
Aging in the upper face can give the impression that a person is tired or unhappy. As no other part of the body so conveys emotion as the eyes, restoring a youthful and aesthetic appearance to the periorbital region can be very impactful to a person’s overall expression. For this reason, forehead rejuvenation can be extremely rewarding for the patient and surgeon alike.
Rejuvenation of the forehead has various interacting elements. These include repositioning and reshaping the eyebrow, improving forehead and glabellar rhytids and lateral orbital crowding, and correcting skin excess over the nasal radix. It is essential not only to elevate the brow but also to restore a full and aesthetic shape, the latter being the more important objective. Because brow ptosis results from an imbalance in the muscles that act on the brow, it is critical to weaken the brow depressors to achieve effective and durable brow elevation. That said, excessive elevation of the brow can create an unnatural, surprised look, and is not an uncommon pitfall in brow rejuvenation surgery. In males, overcorrection of brow position tends also to feminize the appearance of the brows.
To achieve a balanced result, brow rejuvenation is often performed in combination with other procedures. As brow ptosis often accompanies age-related changes of the upper lid, successful periorbital rejuvenation will frequently require a forehead lift in addition to blepharoplasty. Patients with obvious dermatochalasis often reflexively elevate the brow to compensate for eyelid excess, an instinct that can mask underlying brow ptosis. It is important to examine patients in repose to uncover brow descent that will only become more obvious after blepharoplasty if not addressed. The impact that brow position and forehead rhytids have on overall facial aging is frequently underestimated. Patients seeking a face-lift will benefit very frequently from rejuvenation surgery of the upper face to achieve an optimal and harmonious result.
Options for Forehead Rejuvenation
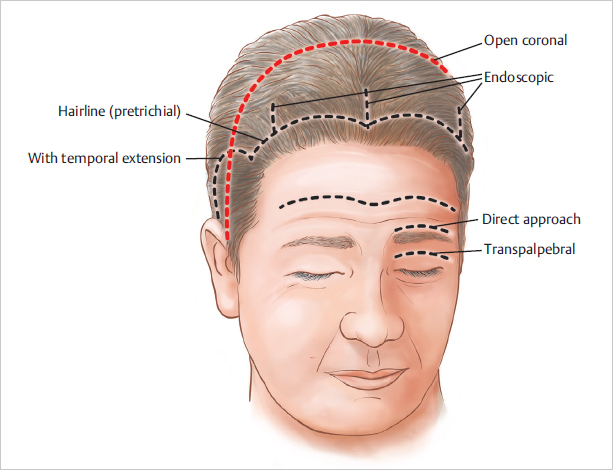
Forehead rejuvenation can be effectively accomplished using various approaches. Neurotoxins can be used to not only elevate but reshape the brow, but its effects are temporary. Surgical rejuvenation can mobilize the brow more durably by modifying the underlying muscles, and in so doing improve upon forehead and glabellar rhytids. Various incisions can be used to access the brow. The surgical approach is selected based on the patient’s anatomy and pattern of aging, his aesthetic goals, and the extent of surgery and scarring he will accept ( Fig. 4.2 ).
Table 4.1 compares various techniques in terms of ease of exposure and effectiveness in mobilizing the forehead and treating the relevant muscles.
Coronal Brow Lift
The open coronal approach provides maximal exposure and thus can be used to very effectively release adhesions, excise muscle, and reposition the brow by a tailored scalp excision. Because of the morbidity of the bicoronal incision, especially the risk of sensory loss and alopecia, this technique is less frequently employed. Nevertheless, a coronal brow lift performed through an anterior hairline incision may still be a favorable option for patients with a high forehead, convex frontal bone, or receding hairline, in whom an endoscopic approach may not be feasible. It is also more effective at mobilizing very thick skin, smoothing deep rhytids, and excising skin excess over the lateral brow or glabella.
Abbreviation: NA, not available.
Note: +, degree of efectiveness is indicated by the number of pluses.
Source: Adapted from F. Nahai The Art of Aesthetic Surgery: Principles and Techniques. 2nd ed. St. Louis, MO: Thieme; 2011.
Technique
Markings
Even with the ample exposure afforded by the open approach, it is useful to preoperatively mark important landmarks such as the temporal crest, sentinel vein, and expected course of the supraorbital and supratrochlear nerves.
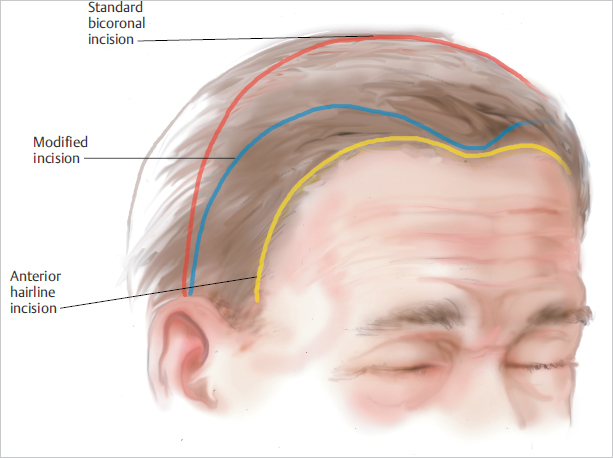
A coronal lift can be performed through a standard bicoronal incision, a modified coronal incision, or an anterior hairline incision. The standard bicoronal incision is situated 6 to 8 cm behind the frontal hairline and can thus be expected to move the hairline posteriorly. While it may be an option for men with low hairlines, it should be used cautiously should hairline recession develop in the future. The anterior hairline incision is used in patients with a high forehead and receding hairline both in the temples and frontal region, as it can be used to reduce the forehead height and advance the temporal hairline. Hairline incisions should be made 1 to 2 mm behind the hairline to preserve some hair follicles anterior to the scar. Incisions can be alternately oriented along hair-bearing scalp and the hairline to correct hairline irregularities, such as a widow’s peak. In patients with a high forehead but normal temporal hairline, a modified coronal incision—one that curves anteriorly in the frontal area—can be exploited to reduce a long forehead ( Fig. 4.3 ). The great disadvantage of hairline incisions is the potential scar visibility.
The proposed vectors of elevation, including one projecting from the peak of the brow, are marked on the forehead preoperatively to guide the scalp excision.
Steps for Coronal Brow Lift
The coronal lift can be performed under local anesthesia, but general anesthesia is preferred, as it is most often combined with other procedures for facial rejuvenation. The patient is positioned supine but with the head slightly elevated to prevent venous engorgement. After washing the hair and parting it to expose the planned incision, the entire field is infiltrated with 0.5% lidocaine with epinephrine 1:200,000, a more dilute preparation to permit use of a greater volume.
At its lateral extent, the coronal incision is made down to the deep temporal fascia, while centrally it is carried deep to the periosteum. It is important to bevel scalp incisions anteriorly above the level of the hair follicles to preserve them and allow their regrowth through the scar. The forehead flap is elevated in a plane between the temporoparietal and deep temporal fascia laterally and in a subperiosteal plane centrally. As the flap is elevated to the orbital rims, periorbital septa and adhesions are released and the glabellar muscles come into view.
When an anterior hairline incision is used, the forehead flap is elevated in a subcutaneous plane, directly over the frontalis muscle. Horizontal forehead lines can be drastically improved as fibrous septa between the muscle and overlying skin are divided. Scalp sensation should not be altered when the dissection is carried out in this plane.
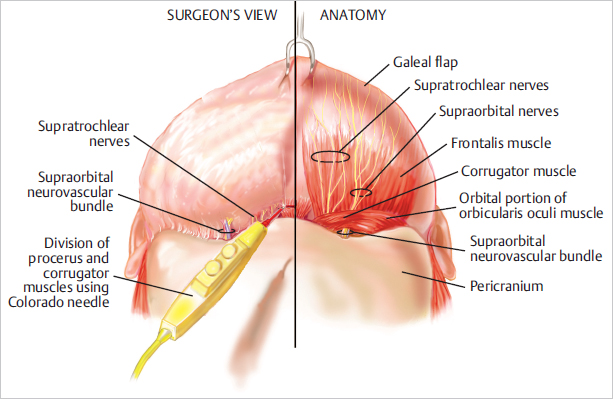
The glabellar muscles, the are divided or cauterized. The frontalis muscle can be weakened by incising its fibers caudally, taking care to avoid the supratrochlear and supraorbital nerves ( Fig. 4.4 ).
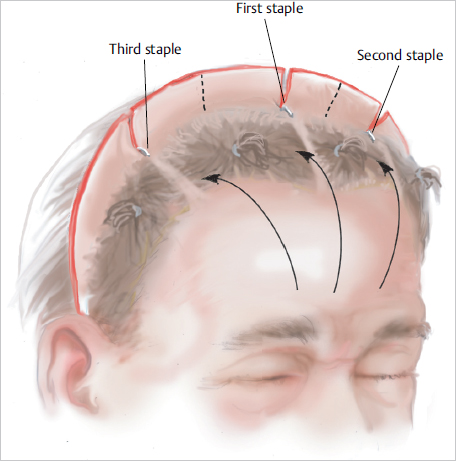
The forehead flap is then redraped and the degree of elevation determined. Darts are created in the flap to secure key points of fixation, generally one at the midline and one on each side. In general, a greater scalp excision is necessary to achieve the desired brow lift, as the heavy male forehead flap will inevitably relax and descend postoperatively. After excising the excess scalp, the wound is closed with galeal sutures and skin staples ( Fig. 4.5 ).
Postoperative Care
The patient’s head is elevated, and ice packs applied to the eyes. Blood pressure is controlled and nausea aggressively treated. If the brow lift is performed in conjunction with other procedures, the patient is generally observed overnight. Skin staples and sutures are removed at 5 to 7 days. Physical activity is restricted for 2 to 3 weeks.
Management of Complications
Possible complications include alopecia and sensory disturbances of the scalp, such as dysesthesias or numbness. Avoidance of tension along the closure and limited use of cautery at the skin edges will minimize the risk of alopecia.
Endoscopic Brow Lift
Introduced by Isse and Vasconez in 1992, the endoscopic brow lift has become an attractive alternative to the coronal brow lift, delivering comparable results with less morbidity and greater acceptance among patients. The shorter recovery time is very appealing to many male patients seeking forehead rejuvenation.
The endoscopic approach can be used to effectively release adhesions and to safely excise muscle, as the endoscope’s magnification generally provides a good view of the supraorbital and supratrochlear nerves. However, because scalp excision is limited, mobilization of the brow and maintenance of brow position rely instead on muscle balance and fixation techniques. The use of fixation is controversial but can be used selectively.
Favorable candidates for an endoscopic forehead lift have a short, flat forehead and hairline that effectively camouflages the scar, that is, one that is stable, nonreceding, and with thick hair. Relative contraindications to an endoscopic approach include a high or convex forehead or a receding hairline. Deep rhytids and excess skin over the lateral forehead and nasal radix are not well addressed with this approach ( Fig. 4.6 ).
Technique
Markings
With the patient seated and clenching his teeth, the temporal crests are marked bilaterally. These points guide the transition from a subperiosteal dissection medially to a subfascial dissection laterally and mark a lateral boundary for the lateral branches of the supraorbital nerves. When visible, the sentinel veins are marked with the patient upright. If not, the patient lays supine, and the veins are marked, as are estimates of the path of the frontal branch of the facial nerve on each side, 1 cm superior to the sentinel vein ( Fig. 4.7 ).
The planned access incisions are marked 1 to 2 cm behind the temporal hairline. The incisions are made over the temporal muscle to ensure the temporoparietal fascia can be anchored to the deep temporal fascia. While the incisions can be oriented in any vector (radial to coronal), a coronal or horizontal incision may be preferable as it allows multiple fixation sutures, while a radial incision accommodates only one.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


