CHAPTER 7 The Male Face-Lift
Summary
Facial rejuvenation in the male patient has become increasingly more common in current day society, where an emphasis is placed on longevity and health. For this reason, many men seek consultation for face-lift with the goal of both looking younger and the potential to remain active in the workforce longer.
Overall, the aesthetic goals and technical principles remain similar between male and female rhytidectomy. These include an unaltered hairline including a natural sideburn length and shape, avoidance of a hair-bearing tragus or surgical alopecia, and creation of a natural-appearing earlobe. Additionally, restoration of a more youthful contour to the neck with elimination of cervical bands and jowling and creation of an acute cervicomental angle are essential.
However, male facial rejuvenation is uniquely challenging for several reasons. First, the male hairline and beard affect incision planning, and operative strategies must account for men’s shortly cropped hairstyles and inevitable future hair loss. Moreover, men inherently have thicker, more hypervascular skin, increasing the potential risk for postoperative hematoma. Last, achieving a natural postoperative result is paramount, since most men do not wear makeup and, in general, prefer a less overdone postoperative result. This chapter will review key differences in the process of male facial aging, the relevant surgical anatomy, and common male facelift techniques.
Introduction
The social and psychological barriers inherent to male rhytidectomy in the past have been replaced by a decrease in stigma and general acceptance of male patients undergoing plastic surgery. Current- day society places an emphasis on physical fitness, health, and vitality. For this reason, men more commonly present to plastic surgeons seeking facial rejuvenation today.
There are several inherent anatomical differences that differentiate male from female rhytidectomy, and make incision planning, operative techniques, and surgical goals unique to the male patient. For example, incision planning is critical in the male patient where a short-cropped hairstyle, potential for future hair loss, and presence of beard and sideburns underscore the importance of thoughtful incision placement. In 1969, Drs. Baker and Gordon proposed an incision across the sideburn, meeting the preauricular incision at a right angle and continuing caudally around the lobule into the postauricular sulcus and onto the mastoid skin. Since then, various modifications have been proposed to better address camouflaging of the incision in the hairline and postauricular regions. The goals of male face-lift today include restoring a youthful appearance, enhancing deep malar and central face volume, preservation of facial hair patterns, and minimization of postoperative hematoma.
Aesthetic and Functional Goals of Male Rhytidectomy
Unaltered hairline.
Avoidance of surgical alopecia.
Creation of a natural-appearing earlobe.
Restoration of more youthful neck contour.
Elimination of jowling.
Creation of an acute cervicomental angle.
Avoidance of hematoma.
Physical Evaluation
The details of the preoperative discussion with the patient are as follows:
Determine the patient’s goals and expectations.
Screen the patient for body dysmorphic disorder or “SIMON” qualities (single, immature, male with overexpectations and narcissism) and, if suspected, refer for psychiatric evaluation.
Discuss current medications. Antiplatelet medications such as aspirin are stopped 2 weeks preoperatively, and generally held until the first postoperative visit.
Discuss planned incisions.
Discuss risks of operation including hematoma, infection, skin sloughing, nerve damage, scarring, and need for further intervention.
Discuss postoperative expectations and recovery.
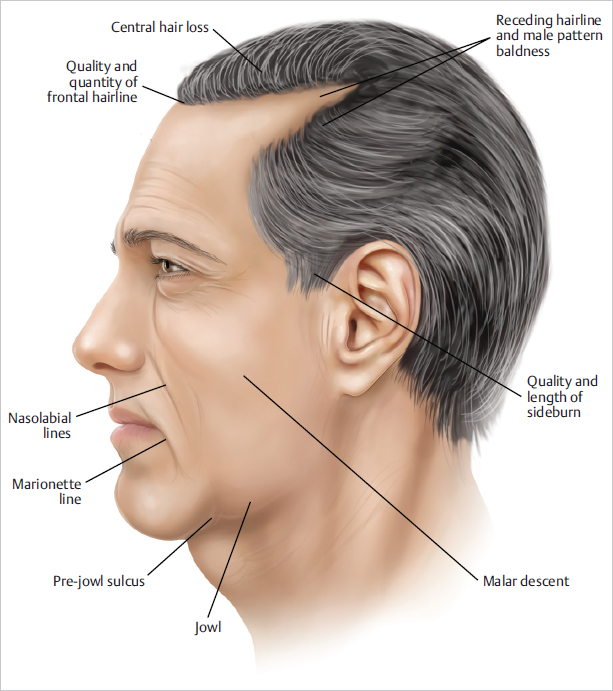
Details of the physical examination are given below ( Fig. 7.1 ):
Evaluate patient’s skin quality, thickness, and laxity.
Evaluate the patient’s hair density, and discuss the patient’s preferred hairstyle including sideburn and bearding patterns. Details specific to the male face-lift include the following:
Men have shorter hair, and less versatility in styling makes camouflaging of the incisions challenging.
The potential for postoperative alopecia must be discussed with the patient.
The patient must understand the possibility of scars becoming visible with natural hair loss. Incision planning in the male patient must account for possible hair loss to prevent subsequent exposure and avoid iatrogenic injury to the existing hair follicles.
Evaluate the upper face for forehead creases, temporal wasting, brow ptosis, and crow’s feet.
Evaluate the midface for lower eyelid skin redundancy, tear trough deformity, and check descent.
Men have a greater amount of central face atrophy.
Evaluate the lower face for severity of nasolabial folds, marionette lines, jowling, submental and neck folds, submental fat, and presence of platysmal bands.
Addressing nasolabial folds, jowling, and neck laxity is central to the male face-lift.
Anatomy
As with female rhytidectomy, an understanding of the relevant facial anatomy including vasculature, retaining facial ligaments, and the location of the facial nerve is critical. There are, however, distinct anatomical considerations in the male face-lift patient to be discussed here.
As previously mentioned, male facial hair patterns are of great importance, and incision planning is guided by hair-bearing skin patterns. As it pertains to the preauricular incision, proponents of the pretragal incision feel that, while visible, the approach prevents mobilization of hair-bearing skin onto the ear. Other surgeons feel that a retrotragal incision is better concealed. If chosen, patients may be asked to abstain from shaving for 48 hours, so that hair follicles redraped over the tragus can be visualized and removed prior to inset. Additionally, the surgeon must be cognizant not to pull hair-bearing neck skin onto the ear when the skin flap is redraped.
Second, the male brow is heavier and flatter than the female brow and is less amenable to surgical manipulation. Overcorrection can result in a feminizing and artificial appearance, and for this reason, concurrent brow lift is performed much less frequently than in female rhytidectomy.
Men additionally have thicker skin, which in the setting of aging-related fat atrophy can act to further deepen nasolabial folds and result in more prominent jowling. Additionally, men have a lower and less prominent malar eminence and a greater degree of central face atrophy. The male superficial musculoaponeurotic system (SMAS) is additionally thicker and necessitates secure fixation.
Last, men often have strong medial platysmal bands and significant neck laxity. For this reason, they generally necessitate creation of a submental incision, resection of preplatysmal and subplatysmal fat, and a greater amount of subcutaneous undermining for adequate redraping.
Steps for Male Face-Lift
This is the author’s preferred method of performing male rhytidectomy.
Preoperative Management and Incision Planning
Preoperative management is critical in the male facelift patient. The patient is met in the preoperative area, where the goals of the operation are reviewed and the patient marked ( Fig. 7.2 ). The location of the surgical incisions is predicated on decreasing their visibility, preventing distortion of natural landmarks, and avoiding any shifting of hairlines. The author prefers a transverse incision at the base of the sideburn at the level of the helical root. Regarding the choice of preauricular incision pattern (pretragal or posttragal), the decision is largely determined by skin laxity, skin quality, and presence of any prior incisions. If the patient has a natural skin crease and no significant sun damage, a pretragal incision may be chosen with care to bevel in line with the hair follicle at the time of incision. Alternatively, a posttragal incision may be made with subsequent defatting and follicular cauterization.
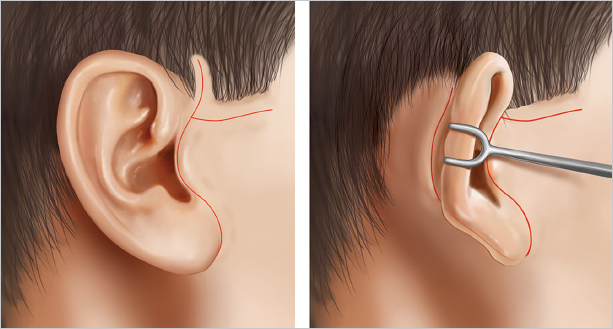
The preauricular incision may be extended superiorly and transversely into the sideburn as needed. The incision is carried caudally beneath the earlobe and into the retroauricular sulcus staying 2 mm on the concha to prevent scar migration onto the visible portion of retroauricular skin. If there is severe laxity of the neck skin, the incision is carried into the hairless retroauricular skin at a point superior enough to remain concealed in patients who prefer a short haircut. In the case of significant neck laxity, the retroauricular incision is continued in the hair-bearing scalp with a sigmoid curve instead of an occipital hairline incision, allowing for shortcropped hair without visible incision ( Fig. 7.3 ).
The planned incision should again be reviewed with the patient after markings have been made. Clonidine may be administered to the hypertensive patient 45 minutes prior to the start of the operation to achieve intraoperative normotension. Once in the operating room, general anesthesia is induced. Tumescent is infiltrated bilaterally and allowed to take effect prior to incision. Additionally, the maintenance of normotension intraoperatively is critical in helping achieve adequate hemostasis.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


