CHAPTER 6 Blepharoplasty: Expert Technique
Summary
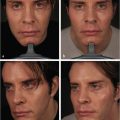
Upper and lower blepharoplasty in men is aimed at reshaping the upper and lower eyelid by removing excess skin and fat. It is important for the surgeon to approach the male patient differently than the female patient, which include minimizing the pretarsal reveal by avoiding a high lid crease and removing excess fat from the superior sulcus thus making a hallowing. For lower blepharoplasty, a transcutaneous approach, leaving some male pattern rhytides, is warranted.
Introduction
Upper and lower blepharoplasty in men is a functional and cosmetic surgical procedure aimed at reshaping the upper and lower eyelid by removing excess skin and fat. In the normal aging process, excess skin on the upper eyelid and fat herniation of the inferior orbital fat are normal as the septum and skin tone weaken with time. This can often give the appearance of a tired, sleepy, and haggard look that patients wish to improve upon through surgical intervention.
It is important for the plastic or oculoplastic surgeon to approach blepharoplasty in the male patient differently than in the female patient to avoid feminization. Several surgical strategies are employed for this purpose. In the upper blepharoplasty, this includes minimizing pretarsal reveal by avoiding creating a high lid crease and not removing excess fat from the superior sulcus so as to make a hallowing. For the lower blepharoplasty, a transcutaneous approach is recommended with a minimal skin trim to leave some male pattern rhytides.
Ultimately, it is important to discuss with the patients what they hope to gain from the surgery and to ensure that each patient has realistic expectations of surgery. While standard surgery on the male patient should not feminize their appearance, there are special cases when a male patient may indeed want to have a more feminine appearance. Thus, every surgery should ultimately be tailored to the individual patient.
Physical Evaluation
Indications for Blepharoplasty
The indications for upper blepharoplasty are, namely, to remove excess skin of the upper eyelids that is contributing to mechanical ptosis, blocking the visual axis, or simply giving the patient a tired look. The goal is also to improve upper eyelid symmetry and upper eyelid contour.
The indications for lower blepharoplasty are to remove excess skin of the lower eyelids and to reduce herniated infraorbital fat under the eyes.
Contraindications for Blepharoplasty
Contraindications for blepharoplasty or when blepharoplasty should be undertaken with caution are in cases of patients with multiple prior eyelid operations, unrealistic expectations, or any pathological condition of the eyelids or orbital structures. These conditions include lagophthalmos, severe keratopathy, upper or lower eyelid retraction, or active thyroid eye disease. Patients who are not healthy, not able to withstand anesthesia, or cannot be taken off blood thinners for cardiac reasons should also not be considered for surgery.
Preoperative Assessment and Patient Selection
The preoperative assessment should include an evaluation of the presence or absence of ptosis. If there is ptosis, this should be further characterized as mechanical or involutional, as the latter would require a concomitant ptosis repair (via an internal or external approach) with the upper blepharoplasty. If the upper blepharoplasty is to be considered functional, a ptosis visual field should be performed to evaluate the degree in which the superior visual field is being compromised. Additional measurements should include the marginal reflex difference 1, the levator function, and the upper lid crease height.
In evaluation of the lower lids, the perceived bags under the eyes should be classified further as festoons or herniated infraorbital fat. In the case of festoons, a lower lid bag will not protrude further in upgaze. This is in contrast to herniated infraorbital fat, which further expands on elevation of the eyes. If the bags are found to be more consistent with festoons, a lower lid blepharoplasty may not be as effective, since there could be another etiology for the edema in this space.
Steps for Blepharoplasty
Upper Blepharoplasty
To begin, outline the area of skin to be excised with a marking pen. Care should be taken to mark the lower incision within the upper eyelid crease to camouflage the scar. Additionally, incisions made above the crease and fold tend to broaden the amount of pretarsal reveal that feminizes the appearance.
Corneal shields should then be placed in both eyes for protection during the procedure. Local anesthesia is then injected into the upper lid.
An incision is made with a No. 15 blade within the upper eyelid crease. Skin and orbicularis muscle are then removed using the curved Stevens tenotomy scissors being careful to stay within the incision line. A strip of orbital septum is then removed across the entire eyelid to access the preaponeurotic fat beneath the orbital septum.
A graded removal of the central and medial fat pad is performed. Contouring of the remaining orbicularis muscle and prolapsed fat is performed with a Colorado-tipped Bovie cautery. Hemostasis is achieved.
The upper lid crease incision is closed in the desired preference of the surgeon. The authors’ method is to use a 5–0 nylon suture in a subcuticular fashion with two to three interrupted 6–0 nylon sutures more laterally. Mastisol with Steri-Strips are then placed over the incision.
Sutures should be removed 5 to 7 days following surgery.
Lower Blepharoplasty
To begin, local anesthesia is injected into bilateral lower eyelids. A transcutaneous approach is preferred in male patients.
A subciliary incision in performed. A skin and muscle flap is dissected down to the inferior orbital rim keeping the pretarsal orbicularis intact. The septum is incised with a Colorado-tipped cautery to expose the herniated fat pads.
Fat is excised in a stepwise fashion over the medial and lateral fat pockets taking care to avoid the inferior oblique.
The skin is temporarily redraped to the original position to reevaluate the lower lid until the desired amount of fat is taken. Then, the lower eyelid skin is redraped and milked temporally to identify a small wedge of skin to be excised. This is done so that any resection is performed over the support of the lateral canthal region to withstand any downward pull from cicatrization. Removal of excess skin is avoided, as this can lead to lower lid retraction.
The subciliary incision is closed in desired preference. The authors close with running and interrupted 6–0 silk suture.
A transconjunctival approach is limited to patients with pure fat herniation, usually in younger patients.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


