Improving Outcomes in Aesthetic Facial Reconstruction
Keywords
• Facial reconstruction • Aesthetic unit • Local flap • Free flap • Skin cancer • Oncology
Facial reconstruction has mesmerized surgeons and the general public alike for many centuries. The earliest descriptions are of cheek flaps and later forehead flaps for nasal reconstruction done in ancient India.1 The pioneering reconstructive work of Esser,2 who at the beginning of the twentieth century was the first to have an understanding of vascularization in “arterial flaps,” was fascinating. Current concepts of aesthetic facial reconstruction have again improved with the development of the aesthetic facial unit principle. The latest frontier in facial aesthetic reconstruction through facial transplantation is currently being challenged.
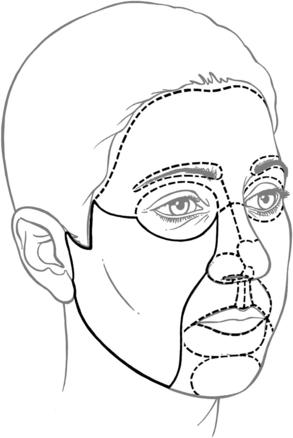
The focus of facial reconstruction has obviously always been restoration of function. With regard to aesthetics, however, facial reconstruction was considered successful when a hole was closed with a flap. Modern facial reconstruction has evolved with the help of detailed anatomic knowledge, which has made tissue transfer from local and distant sites very reliable. In recent decades, the concept of aesthetic facial reconstruction has been popularized. This concept honors the aesthetic facial units, the borders of which are made up of the transitional areas of light and shadow on the face as the facial surface changes from concave to convex (Fig. 1). These borders are the ideal locations to place scars. Central aesthetic facial units, such as nose or lips, can be subdivided into subunits to further refine facial reconstruction.3 The central facial subunits (ie. nose, eyes, and lips) are ideally replaced in their entirety, if feasible, when most of the unit is lost so as to have one inconspicuous reconstructed surface.
One of the cornerstones of aesthetic facial reconstruction is meticulous defect analysis. This holds true for all reconstructive surgery in which a restoration of function is sought. In aesthetic facial reconstruction, however, additional emphasis is placed on the different aesthetic units involved as well as the quality of the tissues and the possible structural support needed by those tissues. This analysis leads to the use of the reconstructive “elevator” rather than the reconstructive “ladder,” in which the flap or combination of flaps are chosen that will give the most aesthetically pleasing as well as functional outcome.4
Functional and aesthetic outcome enhancement by region
Forehead and Scalp
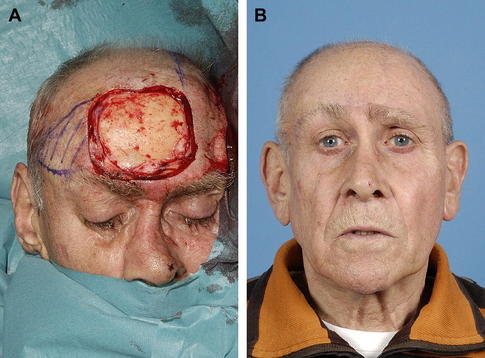
Forehead and scalp reconstruction first aims to cover exposed underlying skull bone or contents. Following successful defect coverage, the main focus of the reconstruction becomes one of a more an aesthetic nature. Successful coverage will not always result in good aesthetic outcome. Small- to medium-sized defects can be reconstructed satisfactorily using local scalp flaps (Fig. 2). In large defects, local tissue will not be of sufficient size to provide coverage, and free-tissue transfer will be required. The main concerns here generally are: (1) coverage that is too bulky or too thin, (2) incorrect skin color, (3) lack of hair, and (4) suboptimal scarring. In addition, sometimes a contour deficiency caused by missing bone may exist. There are a number of solutions to deal with these issues.
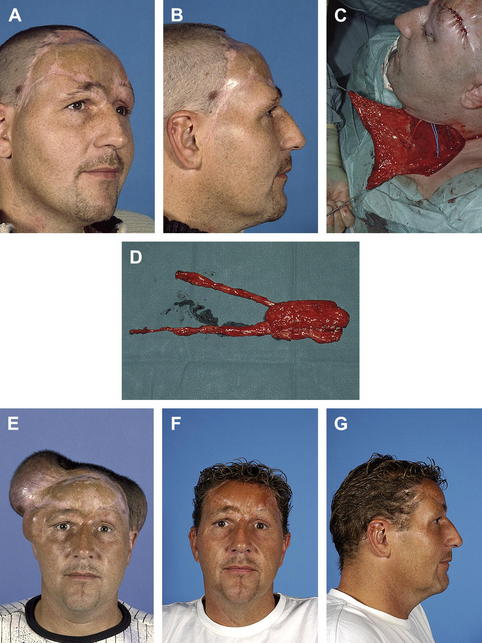
When using a muscle flap with skin graft for coverage, the muscle will thin over time because it is no longer innervated. On the scalp, this will usually not be a major concern. These flaps, however, are less resilient to friction and can present with small areas of skin graft breakdown over time. On the forehead, thinning of a muscle flap can result in a skeletonized appearance, which accentuates the contour of the skull. Correction of this aesthetic problem can be solved by using reconstruction with a regional thin skin flap of appropriate skin color and texture, which, if unavailable, can be generated by flap prefabrication (Fig. 3).
The final skin paddle color of the flap used in a reconstruction is mostly hard to predict. Skin grafts will often change to a different color, which usually is not the color of the surrounding skin. Good results have been reported for skin grafting of the facial area using scalp skin grafts. This is a feasible option for forehead and facial skin reconstruction, but not for larger scalp reconstructions. Alternatively, skin grafting of a de-epithelialized, previously transferred, (distant) free flap using a scalp skin graft may improve skin color match.5




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


