Skin Flaps
Keywords
• Skin flap • Skin transposition • Reconstructive surgery
History of skin flaps
Independently, the Italians developed delayed flaps, tube flaps, and flap transfers by using the upper inner arm skin to reconstruct a nose. This technique was published by Tagliacozzi in the 1500s. In modern medicine, the use of local flaps to repair facial defects began to evolve during the mid-1800s. A variety of flaps were used, but the blood supply and the dynamics of the surgery were not well understood. Harold Gilles popularized tube flaps and flap delays and initiated an interest in reconstructive surgery after World War I.1
Local skin flaps, such as those described in this article, were primarily refined in the 1950s in Europe and the United States by the second generation of plastic surgeons. Ian MacGregor2,3 recognized the importance of an axial blood supply in flap surgery in the 1970s. Plastic surgeons have subsequently redefined cutaneous blood supply. Countless vascularized flaps have since been developed. The skin flaps discussed in this article are primarily random flaps.1–3
Reconstructive options
Healing by secondary intention is a viable option in fixed areas away from important anatomy, such as the middle of the forehead, the cheek, or the neck. In areas adjacent to important, easily deformable anatomic structures, transposition flaps are often a better wound closure approach.4,5
Flap classification
Flaps were first classified as random or axial by McGregor and Morgan3 in 1973. Random flaps had no specific vascular supply. Axial flaps had an arterial and venous blood supply in the long axis of the flap. Further contributions to the classification of flaps were made by Daniel and Williams,6 Webster,7 Kunert,8 and Cormack and Lamberty.9 A random cutaneous flap’s blood supply is derived from the dermal-subdermal plexuses of blood vessels, which originate from direct cutaneous, fasciocutaneous, or musculocutaneous vessels. One example is the rhomboid flap. The arterial, axial, and direct cutaneous flaps are based on septocutaneous arteries. These septocutaneous arteries come either from segmental or muscular vessels, pass through the fascia between muscles, and provide blood supply to the fascia and skin. They also give off branches to the muscle. The cutaneous portion of the septocutaneous arteries runs parallel to the skin surface and has venous comitantes running along with the artery above the muscle. An example is a forehead flap. In summary, survival of the skin flap is dependent on the vascular anatomy incorporated in the flap.10–12
Transposition flaps
Related posts:
 Considerations in History and Physical Assessment of the Plastic, Cosmetic, and Reconstructive Surgery Patient
Culture of Safety
Considerations in History and Physical Assessment of the Plastic, Cosmetic, and Reconstructive Surgery Patient
Culture of Safety
 and Reconstructive Surgery, Ambulatory and Inpatient
and Reconstructive Surgery, Ambulatory and Inpatient
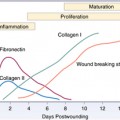 Physiology of Wound Healing: Injury Through Maturation
Physiology of Wound Healing: Injury Through Maturation
 Liposuction
Liposuction
 Antisepsis: First Line of Defense Set Skin Preparation in Motion Before the Incision
Antisepsis: First Line of Defense Set Skin Preparation in Motion Before the Incision
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


