(1)
Klinik für Plastische Gesichtschirurgie, Marienhospital Stuttgart, Stuttgart, Germany
Electronic supplementary material
The online version of this chapter (doi:10.1007/978-3-662-49706-7_10) contains supplementary material, which is available to authorized users.
Keywords
Revision rhinoplastySecondary rhinoplastyDeviated noseCrooked noseNasal pyramidInverted-V deformity10.1 Surgical Principles of Osteotomies in Secondary Rhinoplasty
The principles of nasal pyramid correction in secondary rhinoplasties are identical to the ones in primary rhinoplasties.
The most common reasons for revisions are remaining deviations or asymmetries of the bony pyramid caused by the primary rhinoplasty. These often result from incomplete osteotomies or inadequate postoperative fixations. We think that the postoperative fixation by any kind of cast for only 1 week is often not sufficient.
Therefore, we always change the patient’s cast after 1 week, and often there is the opportunity to correct minor deviations during this time. A cast is applied for a second week, and in patients with a very wide nasal pyramid, we continue to do this for a third week to keep the bony pyramid narrow.
In terms of incomplete osteotomies, the revision has to perform what did not work during the primary procedure. With the technique of external osteotomies, this works nicely.
Another common failure patients complain about is visible stair-step deformities at the lateral nasal wall. These mostly result from a displacement of the osteotomies. If these are performed just at the junction from the nasal bone to the maxilla, the bone transection will always be too high. This happens more often when using the low-to-high lateral osteotomy than in a low-to-low technique; we prefer the latter.
The neglect of the use of spreader flaps or spreader grafts can be responsible for an unpleasant outcome of the primary procedure. Therefore, it is essential to use one of these two techniques in all rhinoplasties in which the dorsum has been lowered. This also helps to prevent the occurrence of inverted-V deformities.
10.2 Case Studies: Secondary Nasal Pyramid Correction
10.2.1 Case 1: Wide Nasal Bridge
A 25-year- old patient presented after three previous rhinoplasties with a wide nasal pyramid and irregularities of the dorsum after grafting with conchal cartilage.
After opening the nose, the anterior septum was found to be overresected. Therefore, a large columellar strut, taken from the septum, was put in a pocket in front of the anterior septal border, and the medial crura were affixed to it. After smoothing the dorsum, paramedian osteotomies were performed with a Lindemann fraise, and then low-to-low lateral and transverse osteotomies were performed transcutaneously. As a result of this mobilization, a satisfactory narrowing of the pyramid was possible. The dorsum was covered with two layers of allogenic fascia (Tutogen). The tip was narrowed by transdomal sutures, and a cap graft from fascia was put on the tip. By using fascia any visibility of the graft was avoided (Fig. 10.1).

Fig. 10.1
(a–c) Correction of wide nasal bridge. Frontal view, profile view, base view pre-op/post-op
10.2.2 Case 2: Wide Nasal Bridge
A 29-year-old patient was seen after two previous rhinoplasties. In addition to a loss of support from overresection of the septum and incomplete lowering of the dorsum, the nasal pyramid was also overly wide. The reason for the deformity of the nasal pyramid was the extremely thick bone, which required four chisels to cut the strong hump. Initially a parasagittal medial osteotomy with a Lindemann fraise was performed after lowering the dorsum, followed by low-to-low lateral and transverse osteotomies transcutaneously to mobilize the pyramid and narrow it. A cast was put on for 3 weeks to guarantee the narrowing of the bones. The missing support was achieved by a strong sandwich graft from the concha. The tip was narrowed by transdomal sutures and contoured by spanning sutures (Fig. 10.2).
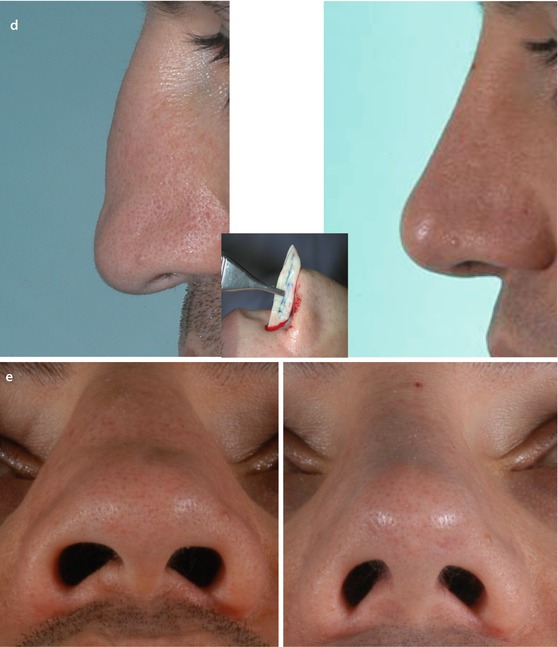
Fig. 10.2
(a–e) Wide nasal bridge. (a) Chisels destroyed by strong bony hump. (b) Strong bony hump. (c–e) Front view, profile view, base view pre-op/post-op
10.2.3 Case 3: Asymmetrical Wide Nasal Bridge
A 51-year-old patient presented after two rhinoplasties, which were followed by nasal trauma. His complaints centered on the deviated nose, an open roof, and a wide tip with asymmetrical nostrils. The facial skeleton was asymmetrical.
The pyramid was straightened and narrowed after parasagittal medial osteotomy and low-to-low lateral osteotomy combined with a transverse osteotomy performed transcutaneously. The dorsum was camouflaged by two layers of alloplastic fascia. Narrowing the tip by transdomal sutures was not effective because of the thick cartilage. Therefore, both domes were divided and then sutured together. A shield graft from the tragus was applied. The residual parts of the tragus were used to graft the supratip area (Fig. 10.3).
Fig. 10.3




(a–e) Correction of asymmetrical wide nasal bridge. (a) Removal of bony spiculae with a chisel. (b) Removal of bony spiculae wth a side-cutting burr. (c–e) Front view, profile view, base view pre-op/post-op
Related posts:





Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
