4 Orthopaedic Evaluation of the Lower Extremity and the Concept of the Orthoplastic Approach
Summary
If salvage of a lower extremity is the chosen path, any reconstruction will require stable skeletal support as well as adequate and durable soft-tissue coverage. The former is within the realm of the orthopaedic surgeon, whereas the latter typically is in the domain of the plastic surgeon or sometimes the orthopaedic soft-tissue expert. Most often, these are complementary roles best performed by a mutual cooperation in using the principles of both specialties to obtain the optimum functional result, and that is the orthoplastic approach. If focusing on the traumatic wound, treatment should be initiated as soon as reasonable, and always after a complete evaluation of the patient for concomitant medical issues. Radical debridement is then essential. If necessary, serial debridement may be required before contemplating closure, and that will be more likely the higher the Gustilo grade of injury. Fracture fixation should be performed so as not to be an obstacle to later soft-tissue management or even vascularized bone transfer. The choice, instead of amputation, must always be individualized, as injury severity scoring systems have been found not to be reliably predictable.
Keywords: orthoplastic approach, Gustilo classification, medial femoral condyle flap, debridement.
4.1 Introduction
Just as in the craft of carpentry, a stable foundation and framework is absolutely essential to uphold the final function of a building, but no more important than the sheetrock, trim, and paint that make the building functional, durable, and livable. Reconstruction of the lower extremity is similar, where the orthopaedic surgeon must obtain stable fixation of the damaged bone while the plastic or orthopaedic soft-tissue surgeon must provide vascularized, stable coverage over that damaged bone. These two components are complementary, not adversarial, and both contribute to the success or failure of functional limb restoration. The quality of bone repair and healing will predict the ultimate weight-bearing status, while the vascularized envelope will bring nourishment, immune system elements, antibiotics, and protection to the repaired bone. When both aspects are properly attended to, the result is often a functional limb with an acceptable appearance. While a single surgeon need not perform both of these tasks (although some may choose to do so), the orthopaedic and plastic surgeons involved in this care must have a clear understanding of the other’s role and the importance of each other for a good outcome. This is what we call the orthoplastic approach to reconstructive surgery of the extremities, that is, the application of the principles of both the specialties of orthopaedic and plastic surgery simultaneously to optimize the outcomes in limb reconstruction.1,2,3,4 We plan to discuss the pertinent history and key elements of orthoplastic surgery along with the factors that lead to good outcomes in lower extremity reconstruction. These will always include a thorough orthopaedic evaluation of the extremity; the role and timing of debridement and then flap coverage; the key elements of bone fixation, limb salvage versus amputation; and other applications of orthoplastic surgery.
4.2 The Orthoplastic Approach
Since the days of Hippocrates, surgeons have treated traumatized extremities by providing fracture stabilization using splints or external fixators, and soft-tissue injuries have been treated with various potions and salves. The need for proper limb alignment and healing of soft tissue and bone has been the subject of medicine throughout both the ancient and modern eras. It is the history of medicine that allows us to introduce the concept of orthoplastic surgery. Individuals such as Ambroise Pare, Gaspar Tagliacozzi, Dupuytren, Velpau, and Malgaigne had careers as master surgeons ranging from the 16th century to the middle of the 19th century. If we read the history of orthopaedic surgery or the history of plastic surgery, each of these individuals is mentioned as founding fathers of these respected specialties.
The evolution of distinct surgical specialties really developed at the conclusion of the 19th century. Modern plastic surgery has its roots in the trenches of World War I and is approximately 100 years old. Probably the first modern orthopaedic plastic collaboration was between W. Arbuthnot Lane and Sir Harold Gilles. In 1919, Lane, an orthopaedic surgeon, wrote the preface for Major Gilles’ textbook, and so began the modern era of “orthoplastic surgery.”4
The development of reconstructive microsurgery allowed modern orthoplastic surgery to develop. In 1960, Jacobsen and Suarez introduced the operating microscope for the suture of small vessels.5,6 In 1968, Tamai reported the first successful digital replantation.7,8 Other microsurgical successes evolved in the later part of the 1960s.5,9 Composite transfer of vascularized tissues became commonplace in the 1980s, with an explosion of techniques, flaps, and the popularization of microvascular surgery not just for the traumatic injury of the extremities and replantation but also for elective reconstructive surgery. Refinements such as flap expansion, prefabrication, and modification of tissue transfers continued to take place in the 1990s.7 During this era, innovations have continued including a better understanding of the angiosome concept and the microvasculature territories of skin, leading to a wide array of new free tissue transfer options for complex defects, for example, by utilizing perforator-based flaps.10 The modern reconstructive microsurgeon today has an armamentarium of flap options: skin, fascia, adipofascial, fasciocutaneous, muscle, or vascularized bone flaps, as well as combined tissue flaps or chimeric flaps. Over the last two decades, vascularized composite allotransplantation has also developed to become the highest rung on the reconstructive ladder.11,12 This explosion of microsurgical advancements has become one of the pillars of orthoplastic surgery.
A better understanding of orthoplastic surgery can be obtained by analyzing the two specialties involved. Plastic surgery specialization over the last 50 years has come to include:
• Microsurgery.
• Hand surgery.
• Burn care.
• Aesthetic surgery.
• Breast reconstruction.
• Craniofacial surgery.
Plastic surgeons tend to place emphasis on:
• Careful soft-tissue handling and reconstruction.
• Detailed suture and layered closure techniques.
• Aesthetics and improving appearance.
Similarly, orthopaedic specialization has occurred with development of separate societies concentrating on:
• Pediatric orthopaedics.
• Trauma.
• Musculoskeletal oncology.
• Joint reconstruction.
• Hand surgery.
• Sports medicine.
Orthopaedic surgeons tend to focus on:
• Functional outcomes.
• Biomechanics.
• Stable bone and joint reconstruction.
• Rehabilitation.
Therefore, the blending of all these strengths of the two specialties constitutes the definition of orthoplastic surgery:
“The principles and practices of both specialties applied to clinical problems simultaneously, either by a single provider or team of providers working in concert for the benefit of the patient.”1,6
This combined “orthoplastic” approach to patients with severe injuries to the lower extremities will lead to not only better outcomes such as quicker time to bone union, more durable soft-tissue coverage, less pain, and better function, but also fewer complications, shorter hospital stays, and higher patient satisfaction, which are all important in the current health care climate of bundled payments and outcomes-based reimbursement, a landmine more easily traversed by always obtaining optimal results.
4.3 Orthopaedic Evaluation of the Injured Extremity
Combined bone and soft-tissue injuries to the lower extremity come in many different shapes, locations, and sizes. The Gustilo classification has become the most widely accepted and simple way to classify open fractures of the lower extremity.13,14 This classification consists of three main categories of open fractures with three subtypes (▶ Table 4.1).
The group from New York University Langone Medical Center has further substratified the Gustilo grade 3B category with a 3–2-1 modification with the numbers stating the total of uninjured source vessels intact in the limb at the initial evaluation.15,16 This better reflects the difficulties to be expected by the reconstructive surgeon, as unplanned returns to the operating room and flap failure rates were found to be significantly greater the fewer the vessels that remained.15 A grade 3B-3 limb with all vessels intact intuitively would appear to have been less injured than a grade 3B-1 limb with only one vessel intact, and therefore the former would be expected to have a superior outcome.
Other key elements of the orthopaedic evaluation of the traumatized lower extremity include1:
• Timing and environment of injury.
• Mechanism and amount of energy absorption.
• Fracture configuration and amount of bone loss.
• Systemic conditions, medical status, other associated injuries.
Table 4.1 The Gustilo-Anderson Classification of Open Fractures
Description | Treatment | |
I | Open fracture, clean wound < 1 cm in length | Irrigation, debridement, ORIF/EF, primary closure |
II | Open fracture, wound > 1 cm but < 10 cm in length without extensive soft-tissue damage, flaps, avulsions | Irrigation, debridement, ORIF/EF, primary closure |
III | Open fracture with extensive soft-tissue laceration (> 10 cm), damage, or loss or an open segmental fracture. This type also includes open fractures caused by gunshot injuries, farm injuries, fractures requiring vascular repair, or fractures that have been open for 8 h prior to treatment | Variable, see below |
IIIA | Adequate soft-tissue coverage of the fractured bone despite the extensive soft-tissue laceration or flaps, or high-energy trauma irrespective of wound size | Irrigation, debridement, ORIF/EF, primary closure, or sometimes requires STSG or local soft-tissue flap coverage |
IIIB | Extensive soft-tissue injury with periosteal stripping and bone exposure. Usually associated with massive contamination | Irrigation, debridement, ORIF/EF, often requires free tissue transfer or local muscle flaps or perforator-based flaps |
IIIC | Open fracture associated with an arterial injury requiring repair, irrespective of degree of soft-tissue injury | Irrigation, debridement, ORIF/EF, vascular repair, often requires free tissue transfer or local muscle flaps or perforator-based flaps |
Abbreviations: ORIF/EF, open reduction internal fixation or external fixation; STSG, split-thickness skin graft. | ||
• Vascularity, sensibility, and motor function of the limb.
• Possibility of compartment syndrome.
Location of soft-tissue injuries along the axis of the leg is also an important factor to analyze. Traditionally, the traumatized lower extremity has been divided into thirds in an algorithmic manner to help guide treatment:
• Upper one-third: gastrocnemius pedicled flaps.
• Middle one-third: hemisoleus pedicled flaps.
• Lower one-third: free tissue transfer.
However, with modern-day microsurgical techniques including perforator-based local flaps such as propeller flaps and reverse flow flaps, and improvement in free tissue transfers, many options now exist for each region of the extremity. A more modern approach to analyzing a lower extremity defect is to focus on the nature of the defect, what is missing and therefore what needs to be replaced, and what local or distant options exist for the achievement of a well-vascularized sealed wound regardless of specific location. However, vital to the success of any reconstruction is the process of preparing the wound by thorough debridement.
4.4 The Role and Timing of Debridement
4.4.1 Timing of Debridement of Open Fractures of the Lower Extremity
Urgent administration of antibiotics is well established in preventing infection of open fractures17 with delays in greater than 3 hours resulting in 1.63 times greater odds of infection.18 However, timing of operative debridement remains controversial. Historically, open fractures were taken emergently to the operating room within 6 hours of injury.19,20,21 However, this practice was extrapolated from data prior to administration of intravenous antibiotics and has been challenged in recent literature. Although most clinical studies challenging the “6-hour rule” have been small retrospective series with fewer than 200 patients,22,23 several prospective studies exist. One such study of 237 patients demonstrated no significant difference in infection rates for operative management earlier or beyond 6 hours.24 In a prospective study of 736 patients, Weber et al demonstrated increasing Gustilo grade and tibia fractures to be associated with a higher risk of infection, but not time to surgery.25 Additionally, several meta-analyses demonstrate no difference in rate of infection with the delay of initial debridement beyond 6 hours.26,27 However, several recent studies still advocate for debridement within 6 hours. One prospective study of 404 patients demonstrated that delayed irrigation of lower extremity fractures beyond 8 hours, higher Gustilo grade, and higher Injury Severity Score increased the risk of infection, but not of the upper extremity.28 In 2009, the British Association of Plastic, Reconstructive and Aesthetic Surgeons revised their guidelines in favor of debridement within 24 hours of injury.
4.4.2 Type of Irrigation Fluid
There is much variation in the manner and content of irrigation solution used in open fractures.17 High as well as low pressure irrigation has been recommended. High-pressure irrigation is thought to be more effective at debriding contaminants from wounds,29,30 whereas those in favor of low pressure have shown high pressure causes potential damage to fractured bone31 as well as bacterial propagation into the soft tissue or femoral canal.32 Yet in 2016, a large prospective multicenter study demonstrated no difference in clinical outcomes with varying pressures of the irrigation solution. They did demonstrate a detrimental effect of using castile soap in the irrigation solution when compared with normal saline.33
4.4.3 Timing of Wound Closure
There are currently no objective clinical guidelines to determine the timing of wound closure.34 Multiple debridements may be required in the case of gross wound contamination or tenuous soft-tissue envelope.17 In these scenarios, delayed wound closure allows for repeated reassessment of the wound, more precise operative planning, and thorough cleansing of the tissue bed.17 Lenarz et al34 instituted a protocol wherein an open fracture underwent serial debridement until cultures were negative before definitive wound culture. Mean number of days to closure ranged from 0.76 for Gustilo grade I to 18.5 for IIIC injuries, indicating that several debridements are often necessary with the increasing complexity of the wound. Using this approach, they obtained an impressively low infection rate of 4.3%.34 Russell et al in an early study found wounds closed primarily after the first debridement had significantly greater risk of infection compared with those closed in delayed fashion (20 vs. 3%).35 However, more recent studies have challenged this approach and have consistently shown that delays in reconstructive wound coverage are associated with increased infection and flap failure rates.36 Godina’s classic work demonstrated that delayed reconstruction beyond 72 hours resulted in an increase in infection rate from 1.5 to 17.5% and a higher free-flap failure rate.37 Fischer et al showed that soft-tissue coverage beyond 10 days of injury was associated with a higher infection rate (18 and 69%).38 Nevertheless, it must be recognized that the magnitude of the soft-tissue damage may affect outcomes. For example, Hohmann et al compared low-grade open tibia fractures and found no difference in the infection rate between primary closure and delayed closure, with a significant cost reduction in the primary closure group.39
In our practice, the following principles of irrigation, debridement, and coverage have proven successful:
• Get the patient to the operating room as soon as reasonably possible (considering vascular status, level of contamination, concomitant injuries, availability of qualified personnel, etc.).
• Perform a “radical necrectomy,” treating the wound as a “pseudotumor” by removing all devitalized soft tissue, bone, and surface contaminated tissue.
• If unhappy with the wound’s appearance (continued bacterial colonization, purulent appearance, or ongoing necrotic or fibrinous debris), take the patient back for a second or third look.
• Irrigation with normal saline at low pressure.
• Use a Versajet for surface decontamination or minor debridements.
• Keep wound moist at all times.
• Negative pressure wound therapy can keep the wound clean and buy more time.
• Early coverage desirable.
• Manage edema.
• Prevent equinus contracture.
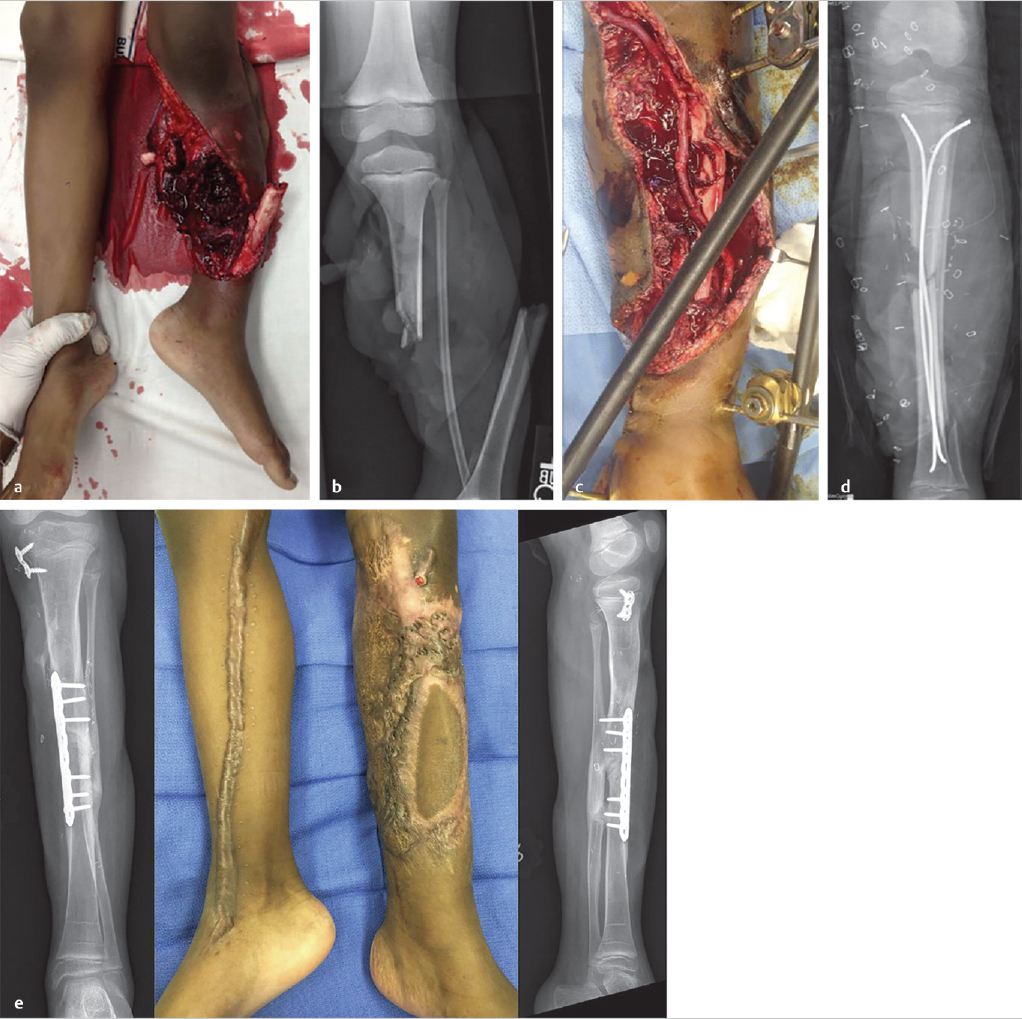
▶ Fig. 4.1 demonstrates a representative case of an 8-year-old child with a Gustilo 3C injury to the lower extremity where these principles were applied. This orthoplastic approach led to successful limb salvage and a good outcome.
4.5 Basic Principles of Bone Fixation
Open fractures with soft-tissue defects necessitate coordinated care to achieve bony union, guard against infection, and maximize functional outcome. In the late 1950s, the Arbeitsgemeinschaft für Osteosynthesefragen (AO) group developed four basic principles for the surgical treatment of fractures. These include:
Related posts:
 General Wound Preparation and Timing
General Wound Preparation and Timing
 Supermicrosurgery Approach to the Lower Limb
Supermicrosurgery Approach to the Lower Limb
 Modern Concepts of Prosthetic Rehabilitation in Amputation of the Lower Extremity
Modern Concepts of Prosthetic Rehabilitation in Amputation of the Lower Extremity
 Lower Limb Vascularized Composite Allotransplantation
Lower Limb Vascularized Composite Allotransplantation
 Using the Flap and Angiosome Concepts to Optimize Functional Lower Leg and Foot Amputations
Using the Flap and Angiosome Concepts to Optimize Functional Lower Leg and Foot Amputations
 Procurement of Thin Flaps as Indicated in the Lower Extremity
Procurement of Thin Flaps as Indicated in the Lower Extremity
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


