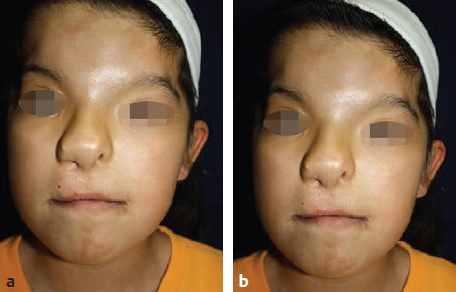
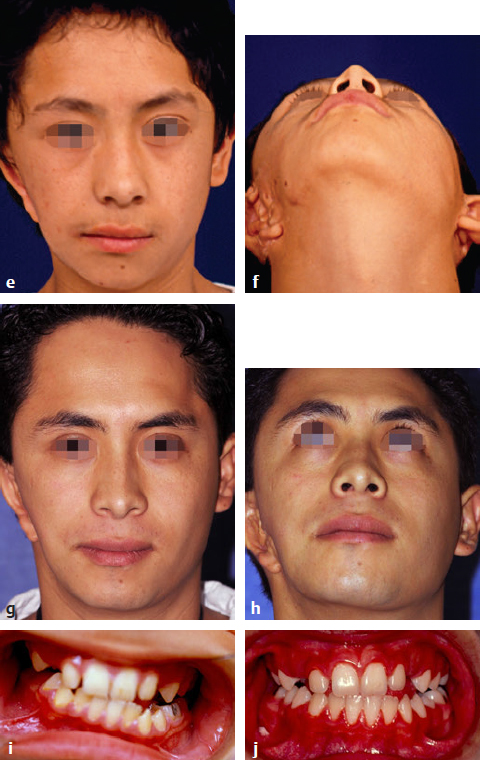
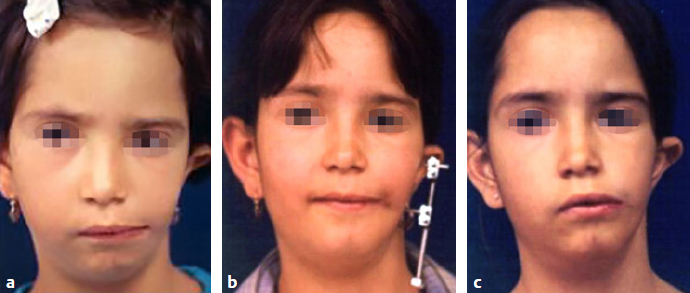
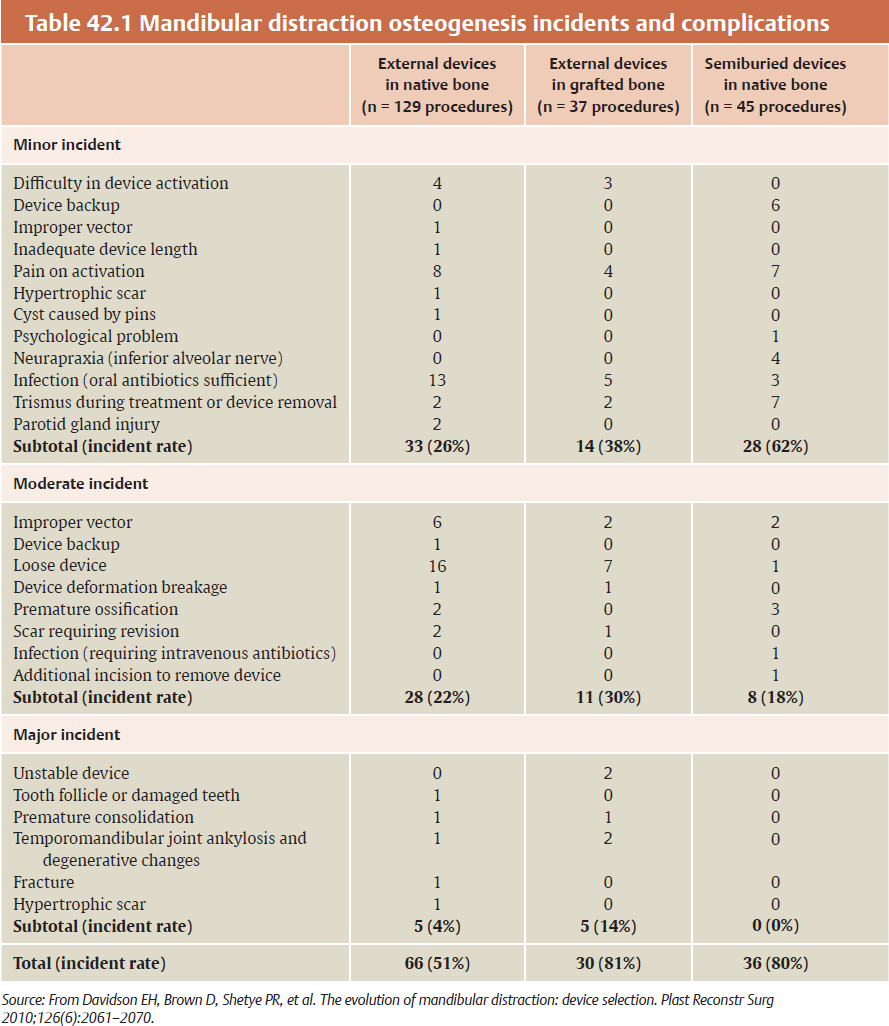
CHAPTER Craniofacial surgeons have the opportunity to offer great possibilities for surgical reconstruction of congenital deformities. Even if these malformations are very complex and include orofacial abnormalities, the surgeon has many different surgical tools, new modalities for planning, and increasingly objective long-term follow-up controls. Ideally the patient’s care should be coordinated by a multidisciplinary team, with different professionals working together to obtain an optimal functional and aesthetic result. Distraction osteogenesis is the treatment of choice for surgical correction of mandibular hypoplasia. The technique represents a significant advancement in the field of craniofacial surgery. Congenital deformities such as hemifacial microsomia, Goldenhar’s and Nager’s syndromes, and Pierre Robin’s sequence may present with mandibular hypoplasia of varying severity.1–4 Mandibular distraction is a less-invasive and less time-intensive technique and has a significantly decreased morbidity rate compared with traditional methods of mandibular reconstruction. Surgeons can generate new bone in patients with unilateral or bilateral mandibular body deficiency, can correct a severe hypoplastic ascending ramus, or can reconstruct a missing condyle in an ankylotic patient. The technique also provides the added benefit of expanding the overlying soft tissues. It likely represents the first tissue-engineering surgical technique to be applied to the craniofacial field. Summary Box Complications of Orofacial and Craniofacial Deformities Hemifacial Microsomia Major Craniofacial Clefts Hypertelorism • Erroneous distraction vector • Incomplete consolidation period • Lack of satisfactory overcorrection criteria • Hypertrophic scar • Loose device • Device deformation breakage • Unstable device • Tooth follicle or damaged teeth • Premature consolidation • Lack of treatment protocol • Lack of preorthodontic and postorthodontic protocol • Hypertrophy or widening of scars • Infections • Canthopexy problems • Dipoplia • Canthal dystopia • Osteosynthesis material removal • Intracranial hematomas • Facial asymmetries • Frontal surface irregularities • Nonsatisfactory aesthetic result • Infections • Brain injury • Cerebrospinal fluid leaks • Anosmia • Major relapse • Postoperative ptosis Bone lengthening and distraction osteogenesis using osteotomies and circumferential gradual distraction were described by Ilizarov and colleagues5,6 to align fractured segments of long bones and to later elongate these bones without a bone graft. Snyder et al7 reported mandibular lengthening in a canine model using an extraoral device. A similar report using intraoral devices followed from Italy.8 More recently, Karp and colleagues9 reported membranous bone lengthening using external devices. Histologic examination of the zone revealed a highly organized biologic process. Since the beginning of the 1990s successful mandibular distraction has been performed on a multitude of patients around the world.10–16 My own experience performing mandibular distraction began in 1990, and I still use a corticotomy and external devices to achieve simultaneous skeletal and soft tissue correction with minimal surgery.17–21 Hemifacial microsomia is the second most common facial birth disorder after cleft lip and palate, with a prevalence of one in 3,500 to 5,600 live births. Facial asymmetry and microtia are the most important clinical findings in a hemifacial microsomia patient. Deviation of the chin to the affected side, hypoplasia of the soft tissues, and associated disorders of other anatomic structures such as the maxilla, the zygoma, and the muscle of mastication are present in a wide variability. The mandibular hypoplasia affects the gonial angle (grade I) in less severe cases and the angle and the ascending ramus in others (grade IIa and IIb); the ramus and the condyle are absent in more severe cases (grade III).22 The surgical procedure consists of three primary components: 1. A vestibular incision is made and the periosteum is elevated. 2. A corticotomy is performed on the lateral, superior, and inferior aspects of the mandible, including the cortex to the cancellous layer. 3. Two pins and an external distractor are inserted. Bone vascularity should be always carefully preserved. Several basic requirements are important when treating hemifacial microsomia with distraction osteogenesis: • Distraction vector is a critical decision. The corticotomy and the position of the pins determine the vector, which varies depending on the grade of mandibular hypoplasia. Oblique, semioblique, and vertical vectors are the most common for patients with unilateral mandibular hypoplasia (Fig. 42.1). • The distraction protocol includes a 5-day latency period followed by a rate of 1.0 mm of elongation per day (distraction period). Bone lengthening produces occlusal changes that must be controlled with orthodontics; posterior bite blocks, dynamic appliances, and other maneuvers are commonly used. Fig. 42.1 (a,b) Preoperative view of a 5-year-old boy who presented with right grade IIa hemifacial microsomia. Microtia and facial asymmetry are associated with a moderate soft tissues hypoplasia at the right side. The hypoplastic angle and ramus in the right side of the mandible is the cause of the deformity. The menton is deviated toward the affected side. (c,d) At the age of 7 years, during the distraction process. A semioblique vector was used for the reconstruction of the mandibular ramus. Initial face changes have begun in the right side. (e,f) The initial result 6 months after the completion of mandibular distraction. Because of the soft tissue expansion at the right cheek, the buccal commissure has descended to the level of the contralateral side. The distance between the lateral canthus to the mouth corner and to the menton has increased. Some volume is lacking on the right side. Mandibular overcorrection after bone regeneration produced the menton medialization and an important leveling of both mandibular angles. (g,h) The result 17 years after distraction. Facial symmetry has been maintained over time. It is still lacking volume on the right side. The patient returned asking for improvement of this volume and definition on the right side of the face. (i) Preoperative occlusion. Orthodontics before distraction included maxillary expansion and intraoral Bionator-style dynamic appliances for 4 months. (j) Occlusion 3 years after distraction. A nice leveling of the maxillary occlusal plane has been obtained. Posterior bite blocks were required to maintain the posterior open bite and to allow the vertical maxillary growth. Dynamic orthodontic appliances also were used to maintain the elongation and to stabilize the occlusion. • Hemifacial microsomia should be overcorrected. This is fundamental for growing patients. Occlusal deformities, impossible to correct with orthodontics, must be avoided when producing overcorrection. Usually, bite blocks are required to maintain the posterior open bite, so the blocks are gradually reduced to allow vertical descent of the maxillae. Ideally, the maxillary occlusal plane should be level horizontally 3 to 4 months after distraction. • The consolidation period is about 8 weeks or more. It depends on the age of the patient and the amount of bone lengthening. More bone elongation requires a longer consolidation period. If the patient is older than 10 years, this period can be extended (Fig. 42.2). • Age of treatment is also a critical factor. Initially the procedure was always indicated at age 5 to 6 years, including the more severe cases. Based on long-term clinical observations, however, if an infant presents with a severe deformity (at least grade IIb), treatment should occur at 3 or 4 years of age, simultaneously with vertical growth of the maxilla. This prevents a constrained mandible, which secondarily affects the growth of the craniofacial skeleton, and avoids facial asymmetry relapse in the short term. Fig. 42.2 (a) Preoperative view of a 6-year-old patient with Goldenhar’s syndrome. She presented with grade IIb mandibular hypoplasia in the left side associated with an ear deformity, severe soft tissue hypoplasia that included the menton muscles, and upper lid coloboma. (b) A mandibular distraction procedure was performed at the age of 8 years with a ramus elongation of 34 mm followed by a consolidation period of 8 weeks. The result after the procedure included restoration of facial symmetry and ear correction. (c) At the age of 12 years, she had a relapse of the deformity. A retrospective analysis of the causes for this secondary deformity revealed a short consolidation period without a complete mineralization of the regenerate and an incorrect distraction vector (rather than a full vertical vector, a semioblique one was used, producing an occlusal deformity that was impossible to correct with orthodontics). Furthermore, the decision to use intraoral or extraoral devices is based on mandibular bone stock. Generally, patients younger than 5 years who have severe or moderate deformity and a limited bone stock are not good candidates for internal distractors. In this group, the procedure fails to achieve the ideal distraction vector and leads to secondary occlusal problems, early relapse, and the need for future surgical interventions. The goal for all patients with hemifacial microsomia is to obtain facial symmetry, with descent of the buccal commissure to the level of the contralateral side and a horizontal menton located at the midline. To produce stability until the patient reaches skeletal maturity, all of the previously listed requirements must be fully addressed. Functional orthodontics should be continued until the patient reaches skeletal maturity. In addition, ancillary procedures such as asymmetrical menton osteotomies, dermal-fat grafts, and fat injections should be included for select patients between 15 and 17 years of age to obtain optimal final results. Nagy and colleagues23 studied randomized controlled trials of early distraction osteogenesis in hemifacial microsomia patients, although statistical evidence to support the use of early distraction osteogenesis for correcting hemifacial microsomia as a single treatment modality is lacking. Unfortunately, the postdistraction requirements (described previously) were not included in this analysis. Once mandibular elongation is completed, additional criteria are responsible for providing good long-term results in hemifacial macrosomia patients. Suh and colleagues24 concluded after 15 years of experience that in their severe patients, the longitudinal results achieved by distraction osteogenesis were unstable and generally led to relapse, although they were very good in the early postoperative period. However, this paper also lacks the methodology analysis of the postdistraction period. I believe there is still a lack of understanding that bone distraction does not change the hypoplastic mandible genetics and growth potential. This malformation includes muscles and other soft tissues as well. Because of this, functional matrix principles do not work correctly. Well-managed functional orthodontics can obtain vertical growth of the maxilla and subsequently assist in satisfactory growth. This fact probably is the most important prognostic factor in the long term. In my experience, 18% of Pruzansky grade IIa and IIb patients require a second procedure. The most common reasons are the following: • Erroneous distraction vector • Incomplete consolidation period • Lack of satisfactory overcorrection criteria In all of these patients, relapse occurs 1 to 2 years later. There is a strong tendency to retake the original ascending ramus shape, facial asymmetry condition, and malocclusion. If the patient is 12 years or older at the time of the second bone elongation, a simultaneous maxillomandibular distraction is indicated. In addition, a complete horizontal maxillary osteotomy should be performed. On the affected side, the pterygomaxillary junction is freed, but it is conserved at the unaffected side to serve as a pivot. Intermaxillary fixation is performed and activation is initiated. The result shows that together with the mandibular elongation, the maxilla follows the bone changes, achieving simultaneous vertical elongation. Occlusal plane slanting varies from 12 to 18 degrees to 1 to 2 degrees after the procedure. Especially in adults, the chin is partially medialized by the distraction. It is not always possible to achieve a normal central position. Therefore this procedure does not eliminate the need for an asymmetrical sliding genioplasty or some extra aesthetic surgical procedures. Free dermal-fat grafts are commonly used for extra volume and mandibular angle definition; fat injection is an excellent alternative to produce volume in the whole hemiface and improve contour, definition, and angularity. Mandibular distraction has evolved from the use of external to the use of intraoral and semiburied devices. Different authors have evaluated the advantages and limitations of various devices, and the perioperative problems and complications have been reported25 (Table 42.1). From their paper evaluating 20 years of follow-up, Davidson and his group25 highlighted the benefits of semiburied devices compared with external devices. They pointed out that semiburied devices reduce scarring and have the mechanical advantages of being applied directly to the bone, being less vulnerable to dislodgment, and being more favorable for a vertical vector. However, their use requires more bone stock, and they have the disadvantage of requiring a second operation for removal. Distraction osteogenesis has simplified the treatment for congenital mandibular hypoplasia. Technically, it is a minor surgical procedure that preserves the integrity of the nerve and vascular supply. The corticotomy and pins produce distraction vectors that allow for vertical and sagittal mandibular elongation that closely follows the normal direction of mandibular growth.10–16 Orthodontics are mandatory; usually a posterior open bite is used at the affected side, and dentoalveolar adaptation and maxillary vertical growth are achieved. In the following years a very satisfactory craniofacial growth can be observed. The simultaneous expansion of the surrounding soft tissue of the face is an additional significant benefit.19,20 Rapid descent of the buccal commissure to a normal position, chin correction, and an increase in the distance between the buccal commissure and the lateral canthus are observed in all cases. During adolescence additional facial volume is required, so dermal-fat grafts and fat injections are commonly used. Chin osteotomies are used for the final refinements to correct facial asymmetry in patients with hemifacial macrosomia. The word face has many connotations. This can be understood in the context of the relationship individuals have with their own faces. Externally, it is their appearance as they would like it to be, whether it is through the eyes of others or the image they see of themselves, reflected in a mirror. Internally it reflects a person’s worth. It is an individual’s dignity and integrity; it is also one’s facade and mask. This inner and outer relationship individuals have with their face is singularly entwined. When a cleft runs through a face, the individual may seem himself or herself reflected in a mirror as shattered. A child born with a craniofacial cleft typically feels a sense of disfigurement and isolation. Regardless of the surgeon’s attempts to restore the physical structure of the face, it is the child who reassembles and reconstructs his or her face from the inside out. Perhaps no other singular deformity distorts the face as much as a cleft. The meaning of the word cleft is apparent and easily understood when one is faced with a clinical example, such as a cleft lip or palate. However, not all defects in the apposition of junctional structures are either as obviously definable as a cleft or as easily classified. Rare or atypical clefts come in myriad patterns of clinical expression. The exact incidence of rare or atypical craniofacial clefts is unknown. Forme fruste and incomplete forms of cleft may go unnoticed. The incidence of common clefts of the lip and palate is better understood. Cleft lip occurs in approximately 1 in 1,000 live births among those of Western European descent.26 The condition is more prevalent in the Japanese population, with 2.1 per 1,000 births,27 and less common in African Americans, with 0.4 per 1,000 births. Davis28 found facial clefts have an occurrence rate of 9.6 per 1,000 for common clefts. Burian29 found an occurrence rate of atypical facial clefts of 24.3 per 1,000. Ortiz-Monas-terio30 reported an occurrence rate of 31 atypical clefts per 1,000 common clefts. Historically, two theories of facial clefting have been described: (1) the classic theory of fusion by Dursy31 and His,32 in which the clefts develop as a result of the failure of fusion of the normally merging facial processes, and (2) the theory of mesodermal migration, which is based on the importance of neural crest cells in the development of the mesodermal component of the craniofacial form.33–35 Attempts to classify craniofacial clefts have a long history in the literature based mainly on clinical and anatomic judgment. Some classification schemes have focused on morphogenesis to explain the mechanism involved in the formation of clefts.36,37 In 1962 the American Association of Cleft Palate Rehabilitation (AACPR)38 classified rare facial clefts into four major groups: 1. Mandibular process clefts 2. Naso-ocular clefts 3. Oro-ocular clefts 4. Oroaural clefts In 1974, at the Interdisciplinary Workshop Conference on Craniofacial Surgery in Chicago, Tessier presented a comprehensive classification scheme of craniofacial clefts. Detailed descriptions were later published in 1976 by Tessier39,40 and Kawamoto.41 This system focused on surgical anatomy and integrating external findings with the underlying skeletal malformation.39 This classification does not attempt to explain the morphogenesis of facial clefts but provides a topographic description that has been widely accepted. It proposes a simplified numeral system from 0 to 14 for all clefts depending on their relationship to the 0 line, which is a vertical cleft of the midline of the face. The palpebral fissures separate facial from cranial clefts. Given the rarity and unique nature of the clinical expression of each craniofacial cleft, treatment plans cannot be standardized; they must be based on the individual assessment of each case. Nevertheless, there are general principles by which the sequence and timing of staged osseous and soft tissue reconstruction can proceed. Only in the mildest expression of a facial cleft can the defect be corrected with a single operative procedure. Early in our unit’s experience, success was defined by repair of a cleft. We closed skeletal clefts with bone grafts. Soft tissue clefts were closed by direct approximation, flap rotation, or z-plasty. The interposition of flaps from different regions of the face produced a patchwork effect because of the differences in color, texture, and thickness of the skin. Z-plasties increased the patchy effect, resulting in scars crossing the face in many directions and inconspicuous locations.42 In reviewing our early results, we realized that we were able to close the fissure in all cases, but our aesthetic results fell short of expectations (Fig. 42.3). Failure to meticulously restore the continuity across the cleft can result in a loss of muscular animation or may leave a persistent stigmata, such as a depressed scar, because of the lack of appropriate soft tissue support. When the regional tissue is believed to be insufficient to allow correction with local flaps alone, an alternative approach is the use of tissue expanders to restore the soft tissue defect with adjacent expanded skin of similar color, texture, and appearance. Patients underwent a total of 1,338 operations, or an average of 2.7 operations per patient. Before the implementation of our current treatment philosophy in 1985, 215 patients underwent 470 operations, or 2.2 operations per patient. The 280 patients operated on with the new treatment philosophy from January 1985 on underwent 868 operations, or 3.1 operations per patient. This includes placement of tissue expanders and all revisions performed under general anesthesia; revisions performed under local anesthesia are excluded. Fig. 42.3 (a,b) Preoperative views of a 4-month-old boy with a very extensive macrostoma. The cleft included the total cheek structure, dividing the parotid gland and reaching the left ear. The facial nerve was intact. (c,d) Postoperative result 1 year after z-plasties were used to elongate the distance between the buccal commissure and the ear. Although the quality of the scars is very good, it extends across the aesthetic subunit of the cheek. Radiographic studies were completed to assess the bone deformity. (e,f) At 4 years of age, he had facial asymmetry with deviation of the chin, inferior lip, and buccal commissure to the affected side. The patchwork appearance of the cheek is a result of the z-plasties. A macrotia is also obvious on the left side. (g) At the age of 7 years, a bilateral mandibular distraction was performed to correct the asymmetrical micrognathia. The body has been elongated more on the left side than on the right. The chin is located at the midline and the mandibular dimension is similar on both sides. (h) At 12 years of age, the facial symmetry has been restored; however, some stigmata is still visible in the form of scars, soft tissue deficiency, lip incompetence, and ear malposition on the left side. In our unit, a series of 495 patients with major cranio-facial clefts were treated43; 65% had multiple clefts and 35% had a single cleft. In 33% of patients, the clefts were unilateral, and in 67% the clefts were bilateral. The treatment objectives were to restore the craniofacial skeleton and reconstruct with skin and soft tissue of like color and texture; this relied on the generous use of tissue expanders. This modern concept was developed by following our patients over more than 4 decades; it became clear that incorrectly placed scars do not improve with time, differences of skin color and texture are permanent, and facial asym metry caused by bony and soft tissue irregularities distracts from an aesthetically pleasing appearance. Now, we always try to obtain the following objectives: • Restoration of the craniofacial skeleton • Reconstruction with skin and soft tissue of like color and texture • Generous use of tissue expanders • Aesthetic unit and subunit reconstruction • Scar location at the limits of aesthetic subunits • Symmetrical repositioning of key facial landmarks In our patients, tissue expansion is used in 64% of all primary reconstructions and in 100% of cases involving total nasal reconstruction. Direct approximation or local flap reconstruction of soft tissues was achieved in 100% of cases, eliminating the need for skin grafts or distant flaps (Fig. 42.4). Fig. 42.4 This 5-year-old boy presented with multiple major facial clefts. He had nasal deformity, right macrostomia, eyelid and orbital deformity, and microtia with mandibular hypoplasia. (a) A frontal tissue expander was inserted for a nasal reconstruction. (b) Postoperatively after nasal reconstruction, iliac bone graft for right ramus reconstruction, and macrostomia repair. (c) At 8 years of age. After radiologic mandibular deformity assessment, unilateral distraction was performed on the residual bone stuck from the iliac graft. A simultaneous telecanthus correction and scar lip revision was also done. (d) Three-dimensional computed tomography was performed at the age of 14 years. At the mandible, the final bone regenerated at the angle and ascending ramus is visible. There was important maxillary vertical growth, almost to the level of the contralateral side. Bone grafts are present in the nasal dorsum. The right orbit has a slight lateral displacement; however, both orbits have a very similar structure. (e) At 18 years of age, the ear reconstruction has been completed and a very reasonable facial symmetry has been obtained after a number of surgical procedures. The results of this study and the associated complications are shown in Table 42.2. Our overall complication rate was 6.2%. Hypertrophy or widening of scars occurred in 18 cases (3.6 %) and was usually located in the region of the lip. Infections occurred in 17 cases (1.3%) and consisted of eight wound infections, seven deep surgical site infections, and two cases of bacterial meningitis. Transnasal canthopexy had to be revised in 11 cases. New-onset diplopia occurred in 6 cases (0.4%), and late-recurrent canthal dystopia occurred in 10 cases (0.8%). Nine patients (0.7%) developed tissue expander problems—five infections and four extrusions—that required its removal. Four patients (0.3%) required removal of osteosynthesis material. Two patients had acute intracranial hematomas that required evacuation, and one patient had a nasopharyngeal bleed that required a return to the operating room for cauterization. There were no perioperative deaths and no cases of perioperative blindness. The overwhelming majority of patients underwent elective operations. However, there were three severe cases of Treacher Collins’ syndrome in which urgent mandibular distraction osteogenesis was used to improve upper airway mechanics and avoid the need for tracheostomy. Twelve patients with upper eyelid colobomas also underwent urgent closure of the colobomas to protect the globe and preserve vision. Of the 30 patients with upper eyelid colobomas in this series, 11 were blind in the affected eye because of a delay in treatment. Twelve patients presenting with large enough colobomas to cause blindness were treated urgently with preservation of vision. Seven had colobomas that were either too peripheral or too small to cause blindness.
42
Orofacial and Craniofacial Deformities
Avoiding and Managing Unfavorable Results and Complications in Orofacial and Craniofacial Deformities
Hemifacial Microsomia
Operative Considerations

Indications for a Second Distraction Procedure
Conclusion
Craniofacial Clefts
Classification
Operative Considerations


Complications
| Percentage of patients | Number of cases (n = 495) |
Multiple clefts | 65 | 321.75 |
Single clefts | 35 | 173.25 |
Complication rate | 6.2 | 30.69 |
Hypertrophy (widening of scar) | 1.3 | 18 |
Infection Wound infection Deep surgical site infection Bacterial meningitis | 1.3 | 17 8 7 2 |
Transnasal canthopexy | – | 11 |
New-onset diplopia | .4 | 6 |
Late-recurrent canthal dystopia | .8 | 10 |
Tissue expander issues Infection Extrusion | .7 | 9 5 4 |
Osteosynthesis material removal | .3 | 4 |
Acute intracranial hematoma | – | 2 |
Nasopharyngeal bleed | – | 1 |
Deaths | – | 0 |
Perioperative blindness | – | 0 |
Total complications | – | 78 |
Short-term solutions for upper eyelid colobomas included an ocular moistening chamber or temporary tarsorrhaphy. Definitive treatment consisted of direct closure, local flap closure, or a lid-switch operation. Of the 66 patients with lower eyelid colobomas, only four were blind and all had corresponding upper lid colobomas. No patient with an isolated lower eyelid coloboma went blind, even in cases of delay in treatment.
All 183 patients who underwent primary reconstruction with local flaps and z-plasties had a secondary reconstruction using expanders and the aesthetic subunit principle, meaning that all scars were located at the limits of aesthetic subunits and facial symmetry was improved significantly (see Fig. 42.4). Only 50 (52%) of the secondary cases achieved reconstruction by aesthetic subunits and were left with scars crossing aesthetic subunits. Tissue expansion was used in 64% of all primary reconstructions and in 100% of cases involving total nasal reconstruction.
Direct approximation or local flap reconstruction of soft tissues was achieved in 100% of cases, eliminating the need for skin grafts or distant flaps. Formal craniofacial osteotomy was necessary in 53% of patients, and 24% required bone grafting to restore the craniofacial skeleton. Bone graft was used on all bony fissures that did not require major craniofacial osteotomies. Most patients requiring bone grafting also required soft tissue work, and these reconstructive procedures were combined when possible. Thus, as with soft tissue work, we completed most bony reconstruction before the child entered school.
Hypertelorism was the most common indication for major craniofacial osteotomy. In 51 cases of median and paramedian clefts, the combination of hypertelorism, anterior open bite, and shortened midface was treated with hemifacial rotation with satisfactory resolution. Hemifacial rotation does not retard midfacial growth44 and thus was performed after age 3 years, at which time the frontozygomatic suture is sufficiently strong, and before the child enters school. In contrast, 64 adolescent patients underwent orbital repositioning by means of orbital translocation.
Optimal timing for intervention remains unclear. Early manipulation of the underlying bony skeleton in the region may potentially disturb normal midface development. Bone grafting of the bony defect early may lock the maxillary segments in place and interfere with the normal direction of growth and remodeling. Although, arguably, the inherent growth potential in these cases remains unknown and may possibly be limited because of the severity of the anomaly, early restoration of the skeletal contour can significantly reduce the deformity and allow the child to be mainstreamed earlier into society. However, what may be an acceptable result at age 5 or 6 years may be less than ideal in the long term.44,45
Because it is especially true that orbital translocation retards midfacial growth, it was delayed in this study until skeletal maturity. Seventy-five patients with mild hypertelorism, Tessier grade II, underwent medialization of the medial orbital walls before entering school. Transnasal canthopexy with 28-gauge stainless steel wire was performed in every case, and the canthopexy had to be revised in 11 cases (22%): four cases of hemifacial rotation, four cases of orbital translocation, and three cases of medialization of the medial orbital walls.
Although the cranial vault grows rapidly in the first year of life, it levels off early. The upper midface grows at a slower rate in infancy but it continues to grow later in childhood and early adolescence. In contrast, the growth of the lower midface and mandible, determined by eruption of the dentition, continues well into adolescence. This overall growth allows the cranio-orbitozygomatic region to reach approximately 85% of its adult size by age 5.46
Consequently, skeletal reconstructive surgery involving the upper midface (cranio-orbitozygomatic region) should be relatively stable after age 5 or 6 years. In contrast, reconstruction of a patient’s maxillary–mandibular complex should be postponed until adolescence, although there are exceptions. Unless significant functional concerns arise, the timing of reconstruction should be based on an understanding of the normative residual growth expected within the operated region of the facial skeleton. Basic principles apply to all facial clefts, but specific problems may arise as individual clefts are addressed.
Conclusion
The laws of normal growth are best formulated and understood when the causes of their exceptions can be established. The experimental method itself rests on the notion that induced and controlled departures from the ordinary can unveil the laws of order. Consequently, the congenitally malformed are nature’s experiment, uncontrolled by intentional human art to be sure, but a source of insight nevertheless. The early teratologists sought to understand malformations by classifying them. The early French anatomists developed three categories: missing parts (monstres par defaut), extra parts (monstres par exces), and normal parts in the wrong places. But a classification is no more than a set of pigeon holes until the causes of the ordering can be specified.
Hypertelorism
Hypertelorism is a descriptive term commonly used to signify any abnormal increase in intraorbital distance.47 Strictly defined, hypertelorism is an abnormally great distance between any two paired body parts; for this reason, Tessier et al48,49 preferred the term orbital hypertelorism, or hypertelorbitism. Telecanthus refers to an increased intercanthal distance, and although telecanthus always accompanies hypertelorism, the reverse is not always true; in some instances, there may be an increased intercanthal distance without true hypertelorism, commonly after facial trauma or blepharophimosis.
During embryologic development, the optic placodes arise laterally and then medially translocate. Hypertelorism results when any condition interrupts this medial movement or when some structure, usually the brain, expands and pushes the orbits apart. The following are the most common causes for hypertelorism:
• Craniofrontonasal dysplasia
• Facial clefting
• Encephaloceles
• Facial trauma
• Craniosynostosis
• Tumors
Frontonasal dysplasia sequence, more common in girls than boys, is the most common cause of hypertelorism. A widow’s peak and broad nasal tip are common manifestations.50,51 The nose is quite broad and truly bifid. Craniofrontonasal dysplasia is a combination of coronal synostosis with frontonasal dysplasia.52,53
Midline facial clefting may be associated with other midline intracranial anomalies. Facial clefting associated with encephaloceles, which may protrude from the cranial cavity through a single or multiple locations, is a very complex deformity. Isolate encephaloceles may be the one exception to the belief that, in all cases of hypertelorism, the distance between the optic canals is normal, or only slightly increased.48
A frontal encephalocele usually exits through the foramen cecum, and a basal encephalocele through the skull’s floor; the midline migration of the orbits is affected, resulting in hypertelorism.
Significant facial trauma most often results in telecanthus, but it may also cause hypertelorism; usually a component of vertical globe dystopia and significant asymmetry accompany the increased interorbital distance.
Syndromic craniosynostosis, particularly Apert’s and Pfeiffer’s syndromes, may present with an increased interorbital distance. Tumors such as fibrous dysplasia and syndromes and Greig’s and Opitz’s syndromes share hypertelorism as a common phenotypic component.
For young adults, the normal values for interorbital distance have been described based on radiologic measurements, between the lacrimal crests.54,55 Giinther56 described the following grading system:
1. First degree (30 to 34 mm)
2. Second degree (35 to 39 mm)
3. Third degree (40 mm or more)
The surgical approach varies based on the severity.
Operative Considerations
Hypertelorism does not always require surgical treatment. In fact, mild hypertelorism is considered by many to be an attractive trait. In addition, the epicanthic folds, exotropia, widely spaced eyebrows, narrow palpebral fissures, and dystopia canthorum may contribute to an illusion of hypertelorism.52
The timing for surgical intervention is based on a number of factors. Babies with encephaloceles may require early treatment for resection of the encephalocele sac. Extreme care must be taken in basal encephaloceles, because they may contain the pituitary gland or the hypothalamus and a gross resection may lead to panhypopituitarism. Children with severe hypertelorism may not be able to develop stereoscopic vision if treatment is delayed.
Surgical treatment at early ages can potentially affect midface growth. However, some reports have suggested that this is only partially true.53–57 It seems intuitive that the larger the surgical procedure and the younger the patient, the more likely that growth centers will be affected, and that subsequent growth will be diminished. Most experienced surgeons will delay surgical correction until a significant amount of growth has occurred, but before any serious psychological issues have had time to develop (usually at 6 to 8 years of age depending on development).
Surgical procedures at a later age will be more stable, resulting in better outcomes. The greater the degree of hypertelorism, the less likely that a single surgical procedure will achieve an optimal final result.
A number of surgical techniques can be used to treat hypertelorism. The cause and the degree for hypertelorism will influence the decision of which technique should be used. Ortiz-Monasterio and Molina55 suggested that surgical correction for telorbitism is essentially an extended rhinoplasty through an intracranial approach. In fact, surgical treatment of hypertelorism is one of the more complex operations by craniofacial surgeons.
The mildest degree of hypertelorism may be treated with subcranial two-wall osteotomies. The two medial walls are then medially translocated after removing a central strut of the nasal dorsum, perpendicular plate, and posterior ethmoid sinuses sufficient to permit medial globe transposition. This medial movement is primarily responsible for distance reduction between the orbits, and in these patients, no significant effect on globe position is observed.
The U-shaped technique (three-wall osteotomy) includes the orbital floor with the medial and lateral walls as a single unit. The osteotomy excludes the orbital roof, obviating an intracranial approach. The nasal airway should be always preserved. The disadvantages of this procedure are the difficulty of the infraorbital osteotomy, the risk of injury to the infraorbital nerve and the lacrimal fossa, and the attempted tooth buds.
“On block” osteotomies are indicated for the most severe cases. In this technique, the orbit is circumferentially cut in the coronal plane posterior to the eye globe equator and a portion of nasal bone, the perpendicular plate, and the posterior ethmoid sinuses is removed. This approach provides complete medialization of the orbits and allows for more significant translocations that may result in a better final stability.
Facial bipartition is usually reserved for children who have any condition with a midline separation of the face (clefts and encephaloceles). An intracranial route is required. In addition to bringing the orbits closer together, the rotational movement of the two lateral facial halves increases the midface vertical dimension and corrects the anterior open bite.56,58,59
Osteotomies are performed in the orbital roofs, medial and lateral walls, and the floors. Instead, a pterygomaxillary dysjunction is performed to allow the maxilla to move in continuity with the orbits. In some patients, the dysjunction may interfere with future midface growth. The larger bone-segment medialization can enhance final stability and preserve unerupted tooth buds. Medial canthopexies are always performed, but the decision regarding bone grafting the nasal dorsum depends on the dorsal height of the paired nasal bones. For children with a significantly increased intraoptic nerve distance, a staged correction should be considered to avoid potential loss of vision. Surgeons without significant pediatric congenital craniofacial experience should only undertake these procedures with the assistance of an experienced surgeon.
Complications
The most common complication after hypertelorism correction is a nonsatisfactory aesthetic result in which the child’s appearance is compromised (Fig. 42.5).
An average reduction between the orbits of 5.3 mm postoperatively (only 2.7 mm between the centers of the globes)60 and an interorbital reduction of 6 mm61 have been reported. Despite these very modest improvements after major surgical corrections, patients and families have reported satisfaction with the results62 (Fig. 42.6).
Infection is one of the more common complications. The infection rate is higher because the required osteotomies must cross sinus cavities. Most craniofacial infections do not present clinically until about 10 days postoperatively, and early antibiotic treatment should be initiated.63
In hypertelorism associated with basal encephaloceles, brain injury is the most common complication. In addition to infections, cerebrospinal fluid leaks, anosmia, major relapse, and postoperative ptosis have been reported; many more serious complications may have gone unreported.57,64–66