18 Orbicularis oris, mentalis, depressor anguli oris
Summary and Key Features
• Aging of the perioral and chin regions is characterized by radial perioral rhytides (so-called smokers’ lines or lipstick lines), decrease in vermilion fullness, inversion of the vermilion, lengthened appearance of the cutaneous portion of the upper lip, downward turn of the oral commissures, pre-jowl notch or sulcus, and chin dimpling. Also, prominence of the labiomandibular (marionette lines), labiomental, and nasolabial folds occurs
• The goal of treatment of the lower face with botulinum toxin (BoNT) is to soften dynamic rhytides through muscular relaxation instead of completely paralyzing the target muscle
• The muscular anatomy of the lower face is complex; therefore caution is advised when performing BoNT injections
• BoNT can be used as monotherapy or as an adjunct to other procedures in lower face rejuvenation
• BoNT as monotherapy can be used for younger patients whose primary concern is not volume loss, but rather fine dynamic and / or static radial perioral rhytides due to muscular activity
• A combination treatment of BoNT and dermal fillers in the lower face has emerged as the gold standard for lower face rejuvenation
Introduction
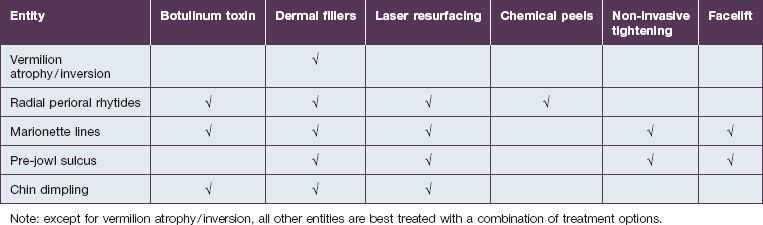
In the lower face, treatment strategies are traditionally focused on volume restoration; however, controlling hypermobility is also essential. Botulinum toxin is used as monotherapy or as an adjunct to other procedures in lower face rejuvenation. Treatment options include dermal fillers, chemical peels, laser resurfacing, non-invasive tightening modalities, and facelifts (with or without chin / pre-jowl implants) (Table 18.1). Although rhytidectomy can reduce the nasolabial and labiomandibular folds, this procedure cannot enhance the lip region owing to its anatomy. The perioral tissues include supportive ligaments that must be preserved, and there is a high risk of motor innervation injury affecting the perioral area through a facelift. This is due to the buccal and marginal mandibular branches of the facial nerve, which course superficially, ramify extensively, and are challenging to identify. Motor innervation injury leads to muscle weakness. A combination treatment with BoNT and fillers in the lower face has emerged as the gold standard because it addresses a broader spectrum of facial aging changes, without the need for surgery.
Anatomy
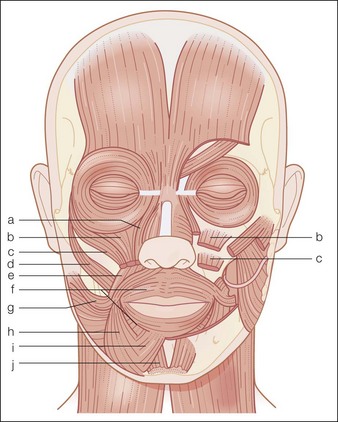
The musculature of the perioral and chin area is complex and includes the orbicularis oris, risorius, DAO, zygomaticus major, zygomaticus minor, levator anguli oris, levator labii superioris, levator labii superioris alaeque nasi (LLSAN), depressor labii inferioris, mentalis, and the platysma (Fig. 18.1).
Perioral and chin aging
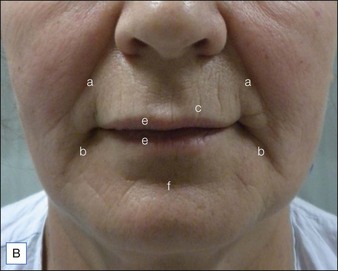
Aging of the perioral and chin regions is characterized by radial perioral rhytides (so called smokers’ lines or lipstick lines), decrease in vermilion fullness, inversion of the vermilion, downward turn of the oral commissures, lengthened appearance of the cutaneous portion of the upper lip, pre-jowl notch or sulcus, and chin dimpling. Additionally prominence of the labiomandibular (marionette lines), labiomental, and nasolabial folds can occur (Fig. 18.2A,B).



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


