17 Treatment of the mid-face with botulinum toxin
Summary and Key Features
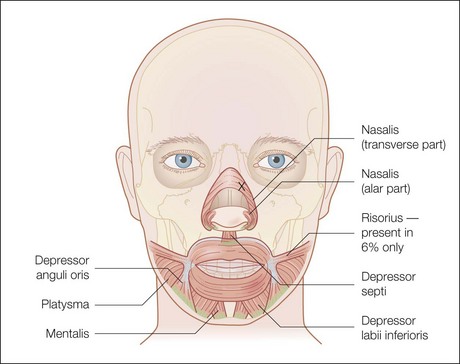
• The mid-face is an area of complex muscular anatomy, with intimately associated, small muscles
• Proper function of these muscles is essential for accurate emotional conveyance, and particularly smiling. Smile dysfunction can be profoundly disfiguring
• Small starting doses are necessary in the mid-face to obtain desired results and avoid overtreatment, and all precautions should be taken to maximize proper placement and minimize diffusion
• Careful patient selection and full exploration of the risks and benefits of treatment should occur before botulinum toxin injection in this area
Introduction
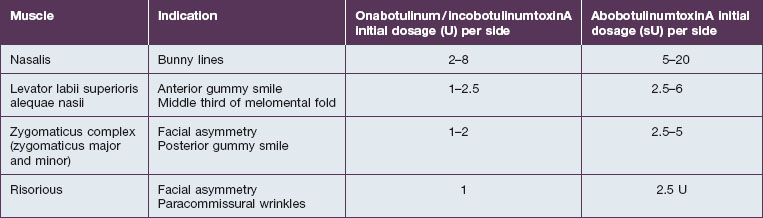
The smaller mid-facial muscles require smaller doses when compared with their upper facial counterparts, especially in initial treatments. The advent of multiple botulinum toxin formulations has added another layer of complexity to this already challenging application and it is important to be aware of proper conversions / dilutions for each toxin (Table 17.1). Small errors in absolute dosage make a large difference in the percentage of the intended doses in this area. The activity of onabotulinumtoxinA (Botox®) and incobotulinumtoxinA (Xeomin®) is measured in murine lethal units (U), with both agents available as 50 U or 100 U per bottle with unit equivalency. It is best to use a higher concentration (e.g. 100 U/mL for Botox®) in the mid- and lower face to minimize toxin diffusion. Abobotulinum toxin A (Dysport®) activity is measured in Speywood units (sU) with either 500 sU or 300 sU/bottle, with a typical dilution of 250 sU/mL. As such, onabotulinum / incobotulinum toxin units and abobotulinum units are not interchangeable, and the exact conversion factor is controversial. According to FDA-approved labeling for the treatment of the glabella, 1 U Botox® is approximately equal to 2.5 sU Dysport®. However, studies have found abobotulinumtoxinA : onabotulinumtoxinA unit ratios to be in the range of 2.5–5 : 1. Some studies such as that by Husseman & Mehta have found abobotulinumtoxinA (Dysport®) to have greater diffusion than onabotulinumtoxinA, meriting even additional caution given the intimately associated nature of the muscles in this area.
‘Bunny’ / nasal sidewall scrunch lines
Injection sites / dosage
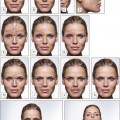
Injection sites for bunny lines are highly individualizable, as are the patterns of the lines. In general, one should ‘inject the fold’ within the following parameters. Injection sites should be kept high on the lateral nasal sidewall (Fig. 17.1) and well medial to the nasofacial sulcus to avoid inadvertent LLSAN weakness. Injections need to be placed only superficially (i.e. intradermally, raising a bleb) to avoid increased diffusion in the low-resistance subnasalis plane. The typical dose ranges have been reported as 2–8 U for onabotulinumtoxinA on each side or 10–20 sU for abobotulinumtoxinA. Figure 17.2 shows a patient before and after bunny line treatment. If LLSAN has a large role in the formation of bunny lines, and the patient is a candidate for LLSAN treatment (as discussed below), that area can be treated concomitantly.