12 Glabella
Summary and Key Features
• Botulinum toxin type A for treatment of glabellar rhytides was FDA approved for cosmetic use in 2002, but has been used for this purpose for over 20 years
• Injection of botulinum toxin into the glabellar complex (corrugator supercilii and procerus muscles) and the lateral eyebrow may achieve reduction of glabellar rhytides and lower forehead rhytides, and brow lift
• There are currently three types of botulinum type A toxin injectables specifically FDA approved for the treatment of glabellar furrows, including Botox®, Dysport®, and Xeomin®, at doses of 20 units (U), 50 U, and 20 U respectively
• Dose variation may be required to obtain optimal correction and higher doses may be required in men
Introduction
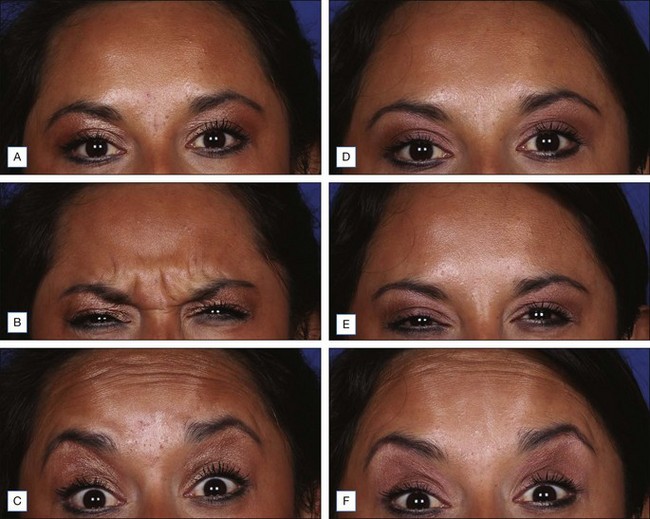
The use of botulinum toxin type A over the last two decades for treatment of glabellar rhytides has revolutionized the field of cosmetic dermatology and plastic surgery. Several multicenter, double-blind, randomized, placebo-controlled studies have proven its efficacy (e.g. that by Carruthers et al in 2003). It is the first quick, less invasive and effective, non-surgical technique for both brow lift and rhytid treatment. The same group demonstrated in 2010 that botulinum toxin type A injection to the glabella has been shown to improve both dynamic glabellar rhytides and those in repose. Subsequent uses of botulinum toxin type A for cosmetic improvement of forehead, perioral area, chin, crow’s feet, and other rhytides have been successful, but its use in the glabella is the first and still the most widely used.
Anatomy
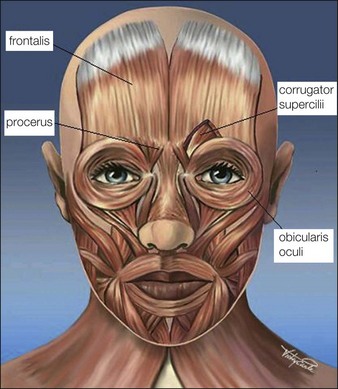
The glabellar complex consists of the two corrugator supercilii muscles and the procerus muscle that collectively serve upon contraction to pull the brow medially and downward (Fig. 12.1). The corrugator supercilii are two sets of horizontally oriented muscle fibers that lie beneath the medial eyebrow to about the mid-pupillary line. In some patients, the corrugators extend beyond the mid-pupillary line (these muscles can be visualized at maximum contraction when ‘frowning’). The procerus is a vertically oriented muscle that lies in between the eyebrows. The frontalis muscle of the forehead is vertically oriented and the medial belly interpolates with the glabellar complex, and its lateral portion interpolates with the lateral orbicularis oculi. Its main function is to elevate the brow. The orbicularis oculi is a thin circular muscle around the eyes that lies on top of the lateral portion of the corrugator supercilli. The lateral portion of the orbicularis oculi under the tail of the brow is a powerful brow depressor upon contraction. The levator palpebrae muscle lies beneath the orbicularis oculi, underneath the bony orbital rim, and its function is eyelid opening. Rhytides are typically perpendicular to the orientation of muscle fibers, thus contraction of the glabellar muscles typically produces vertically oriented lines between the brows.
 Injection technique (see Video ‘Botulinum Toxin Glabella’)
Injection technique (see Video ‘Botulinum Toxin Glabella’)
The proper preparation, storage, and handling of botulinum toxin is discussed in Chapters 9 and 11. Insulin syringes or 1 mL syringes with 30–32 gauge needles are typically used for injection.
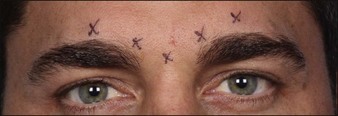
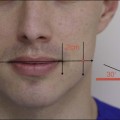
In the glabella, there are typically five injection sites: one at each medial corrugator, one at each lateral corrugator (1 cm above orbital rim at the mid-pupillary line), and a single injection into the procerus (Fig. 12.2). For some patients with particularly long or stronger corrugator muscles, an additional injection site may be given midway between the medial and lateral corrugator injection sites (a total of seven injections).