Oncoplastic Breast Surgery and Shared Decision Making
Maurizio Bruno Nava
Nicola Rocco
Giuseppe Catanuto
History
Surgical treatment of breast cancer has moved from a simple unique decision (Halsted mastectomy) to a high number of possible techniques. Multiple biologic, topographic, and morphologic elements drive the final decision. Moreover, surgery should integrate with other treatments such as radiotherapy (RT) and systemic drugs (1,2,3). Finally, all these elements should be discussed with the patient and a shared decision should be reached. Notably, in our previous report we demonstrated that our decisions’ pathway receives the highest amount of information from the patient. We also proved that every decision can be adapted to personal and disease-related necessities (4,5).
Shared Decisions and Breast Cancer
Medical decisions have become even more complex nowadays. Very often, several different therapies can be offered to treat the same disease. These may be associated to various side effects that can be temporary or irreversible.
Surgery, by definition, determinates irreversible changes. In similar conditions, the participation of patients in the decision process becomes mandatory and this is the case of breast cancer surgery (5). Mastectomy, for example, is a permanent mutilation of an apparently useless organ. For this reason, some patients refuse complex treatments and still consider this technique the most simple and suitable decision.
Patients affected by breast cancer requiring surgery may benefit the most from the shared decision approach, as decisions are particularly complex and multifactorial. The breast is the most important landmark of female identity and therefore any scar, mutilation, or amputation needs to be discussed and managed according to personal values (6).
Not only patients but also the healthcare system benefits from shared decision making (SDM) with an increase in its efficiency (7). Legare (8) who confirmed that 20% of patients who participated in SDM choose less-invasive surgical options proved this. Another study from the Group Health (9) demonstrated that decision aids determined about 32% less surgery for hip and knee replacement with consistent savings across 6 months (10,11).
A study from Budden (12) concluded that women not involved in the SDM were also less likely to be satisfied with the decision process (assessed using the Treatment Decision Satisfaction Questionnaire and the Brief Symptom Inventory-18). There is a demonstrated link in this study between psychological distress and somatization and poor participation in SDM. The relationship between patient’s involvement and outcomes was analyzed also by Janz (13).
An active role was associated to higher satisfaction with decision, a higher education level generated a more active role, and patients who had more self-efficacy in communication had more influence in the decision process. Some studies investigated the role of SDM strictly according to surgical strategies. More mastectomies were associated to a higher patient’s involvement by Katz in a subanalysis of the Surveillance, Epidemiology, and End Results (SEER) database (14). Despite it being clear that surgeons supported breast-conserving surgery, well-informed patients surprisingly decided to remove the entire gland. The authors speculated that this decision might be conditioned by fear of recurrence and by the preference for avoiding radiation treatment. More recent information from evidence at high level can be used to reassure patients about these issues and encourage breast conservation whenever is possible (15). Regarding breast reconstruction, it is interesting to note that this choice is also associated to levels of beneficial interaction between patients and doctors (16).
General Concepts of SDM Applied to Oncoplastic Breast Surgery
The model proposed by Elwyn (17) for SDM translates complex conceptualization into a practical tool for everyday clinical work. A three-step process is designed to let the patients move “from initial preference” to “informed decision.” In the original work by Elwyn the step one of the clinical tool is called “choice talk.”
During this phase the physician communicates about the diagnosis, the characteristics of the disease, the amount of known information related to the actual condition, its prognosis, and the possibility to be treated in several ways. At this stage, the patients should know that different treatments may have different consequences and that some of these might matter more to them than to other people. Moreover, side effects are variable on individual basis and treatments may be unsuccessful. Before starting an interaction at this stage, it may be helpful to check reactions and prevent the request of an immediate and premature closure of the entire process.
The second stage of the process is called “option talk.” During this an investigation of the actual level of patient’s knowledge about various options should be performed. A list of possible alternative solutions can be offered and these should be evaluated in details in terms of harms and benefits. After a brief summary the final phase will start.
The “decision talk” should focus on preferences of the patients. At this stage, a preference could be elicited bearing in mind that a backup option should be available. After this, we can move to a decision although the doctor should always keep a door open to any change.
This original model was criticized because of possible overlap in the first two phases. The first phase (choice talk) was then changed in 2017 (18) and denominated “team talk.” During this phase patients and doctors discuss and deliberate an alliance to make a final perfectly suitable decision. During the following phase, each possible alternative has to be discussed in terms of harms and benefits. An active comparison in view of patient’s principles is expected at this stage. After discussion of possible options a decision has to be taken.
Preliminary Phase
To adapt the three talks model to the oncoplastic work, we added a preliminary phase in which we collect factual, objective information on disease and patients’ characteristics.
Patient’s Personal History and Morphologic Characteristics
Several aspects of personal history affect the final surgical decisions. For instance, patients with a family history of breast cancer, when a gene mutation is demonstrated (19) can be offered a bilateral mastectomy for prophylactic purpose. This may happen even in case of small unifocal lesions otherwise treated by breast-conserving surgery.
General conditions, age, and comorbidities play a role in options’ selection. For example, elderly patients with hormone-responsive disease not candidate for surgery under general anesthesia, whose lesions are too wide to allow local anesthesia can be candidate to preoperative systemic endocrine treatment and surgery can be delayed until this can be performed in safer conditions (20).
Other conditions may interfere with surgery, for instance, heavy smokers may risk necrotic complications (21) as well obese patients and diabetic (22). Previous surgical procedures may interfere with autologous reconstructions whereas any other surgery to the breast followed by RT could increase the complication rates and interfere with therapeutic decisions.
During the first consultation, before communicating the diagnosis and treatment plans, patient’s morphology has to be assessed. The original oncoplastic workflow included only breast volume and ptosis, but with more generalized use of autologous tissue and fat transplantation, we advise to estimate distribution of fat in other regions of the body, morphology of the lower abdomen, and presence of scars.
Regarding breast volume, we do not use any quantitative estimation. This can be rather intrusive (except for 3D photography that is poorly validated and expensive) thus we prefer to rely on bra cup size. Ptosis is classified according to Regnault classification (23).
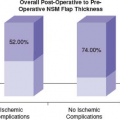
Assessment of body mass index can partially assist in identification of risk factors and surgical choice. In this phase modern imaging can provide useful information not only for diagnosis and staging of disease, but also for surgical planning. We use digital mammography to anticipate thickness of mastectomy flaps and risk of necrotic complications during nipple areolar complex (NAC)–sparing mastectomy and direct-to-implant (DTI) breast reconstructions (24,25). Other studies demonstrate that pattern of skin vascularity (as observed during contrast-enhanced MRI) may provide useful information for the safe surgical planning of breast reconstructions (26).
Assessment of Disease Characteristics
Breast cancer is a heterogeneous disease. A very basic histologic classification identifies in situ and invasive cancers. Intraductal cancers are generally treated with primary surgery. This can be breast conservation or mastectomy according to extension of disease. Excisions in this case should be planned in order to leave 1 to 2 mm of free margins (27).
Post–breast-conservation RT has proven to be beneficial in reducing invasive recurrence (28,29). There are no randomized trials comparing breast-conserving surgery to mastectomy in this setting. The need of post–breast-conservation RT could be avoided in selected conditions and this should be communicated to the patient. Invasive cancers, by definition require systemic treatment. Generally, this is planned according to a surrogate classification of molecular subtypes or using gene-based recurrence score (such as Oncotype Dx) (30) that indicate risk of recurrence and benefit from chemotherapy (31,32). The information on surrogate subtypes should be
available before surgery as this can indicate primary systemic therapy (chemotherapy+/− target therapies or hormonal therapy in selected conditions).
available before surgery as this can indicate primary systemic therapy (chemotherapy+/− target therapies or hormonal therapy in selected conditions).
Some trials in the past demonstrated that systemic treatment before surgery can downsize unifocal cancers and allow breast-conserving surgery or can allow radical surgery in locally advanced breast cancers. Some authors (33) demonstrated that despite a higher chance of pathologic complete response with modern therapies breast-conservation rates are not increasing. For these reasons patients should be informed properly on the purpose of systemic therapies administered before surgery.
Clearly the most important driver for surgical decision is the local staging of disease. Cochrane et al. demonstrated (34) that there is a clear relationship between tumor size, location, and cosmetic results. This is expressed by a ratio that can be calculated using digital mammography. Clearly not all lesions are unifocal, some may be extended to other quadrants, or may be associated to microcalcifications. All this information should be addressed before any final decision and should be derived from clinical examination and imaging including MRI scans. In any case surgical removal has to be designed with radical intent.
The combination of biologic, morphologic, and topographic information generates multiple therapeutic choices with an expected equal oncologic outcome but different side effects. The patient is invited to select the strategy that better fulfills her needs and expectations.
Before calling for decisions, the surgeon still needs to identify subsets in which a mastectomy is invariably required (extended DCIS, locally advanced breast cancer, multicentric or multifocal disease not suitable for breast conservation due to poor tumor-to-breast ratio). It is debatable if in borderline conditions breast-conserving surgery has to be offered as in the form of therapeutic mammoplasties (35) or in any kind of breast-conserving surgery with uncertain radical intent or with positive margins.
It is advisable to have a defined plan before starting the three steps of the SDM.
Shared Decision Making Before Oncoplastic Procedures
Team Talk
During the step one of the SDM the surgeon seeks an alliance with the patient. In this phase we explain that breast cancer is a very curable disease especially at early stage. Survival is not really threatened by surgical decisions provided that surgery is radically performed. Thus life after diagnosis and treatment in most of the cases is not in threat, on the contrary quality of life (QoL) is likely to be influenced by poor initial decisions on treatment. During the initial talk the physicians should involve the other caregivers provided that the patient is keen to accept support from them in the decision process. We find it determinant in this phase that doctors should use a very easy language. Sometimes even well-educated patients can find medical terminologies hard to understand. In this phase we should inform patients about uncertainties related to every kind of treatment (i.e., treatment of breast cancer is multidisciplinary; multiple pathways of treatment may reach the same goal, each treatment has different consequences; sometimes treatments are not effective or may generate side effects of different magnitude). The doctors should be able to check patients’ reactions and avoid premature closures. Several barriers become evident during this phase. Until recently for instance, patients still believe that they should do what doctors think is best.
Option Talk
The proper information burden to patients:
The information on oncologic effects of surgical procedures: The wider the resection the better the oncologic outcome: False! Inform patients that wider resections are not required for therapeutic purposes.
Despite surgery still being the most practiced primary treatment of early-stage breast cancer, systemic and local–regional therapies are effective in reducing significantly the disease recurrence (local or systemic) and minimizing extensive resections.
For these reasons, wide free margins for invasive cancers have been replaced by the no-ink-on-tumor policy for invasive cancer and narrow margins for DCIS. This policy is a widespread standard for breast conservation nowadays (38).
Related posts:
 Patient Selection for Breast-Conservation Therapy
Patient Selection for Breast-Conservation Therapy
 Oncoplastic Approach to Maximizing the Lumpectomy-Level I
Postneoadjuvant Axillary Assessment and Management
Oncoplastic Approach to Maximizing the Lumpectomy-Level I
Postneoadjuvant Axillary Assessment and Management
 Optimizing Mastectomy Flaps Based on Breast Anatomy
Optimizing Mastectomy Flaps Based on Breast Anatomy
 Liposuction as a Viable Treatment for End-Stage Upper Extremity Lymphedema
Liposuction as a Viable Treatment for End-Stage Upper Extremity Lymphedema
 Oncoplastic Techniques in Breast Conservation Therapy—The Plastic Surgeon’s Perspective
Oncoplastic Techniques in Breast Conservation Therapy—The Plastic Surgeon’s Perspective
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


