Introduction
The omentum flap was one of the first free flaps reported in the literature but long before that, its use as pedicled flap for intra- and extra-abdominal reconstructions was well described. The popularity of the omentum flap has been variable over the past decades but new harvesting techniques have been developed that aim to reduce donor site morbidity.
In recent years, the superior epigastric flap has become a versatile perforator flap for coverage of locoregional defects. The concepts of angiosomes and perforasomes led to a better understanding of vascular territories, to a safer flap harvest, and therefore to an increased use of this fasciocutaneous flap.
The external oblique and the internal oblique muscle flap share not only similar characteristics but also the same dominant source vessel. They can be used as both free and pedicled flaps.
Omentum Flap
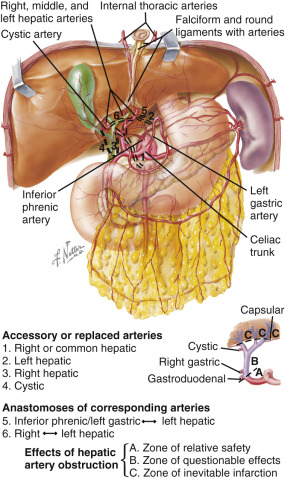
Flap Anatomy ( Fig. 36.1 , see also Ch. 38 )
Arterial and Venous Supply of the Flap
The blood supply to the omentum flap is equally provided by the right and the left gastroepiploic vessels. As the diameter of the right gastroepiploic artery is usually bigger than the one of the left side, the flap is preferably based on the right gastroepiploic vessels. Additionally, extensive dissection of the left gastroepiploic vessels may carry the risk of inadvertent injury to the spleen. The intra-abdominal arcade has four major branches: the accessory omental artery, the right omental artery, the middle omental artery, and the left omental artery. The middle omental artery anastomoses with the left and right omental arteries. This is an important consideration when the flap design requires lengthening of the omentum or splitting of the flap into several parts.
Dominant:
right gastroepiploic artery
Length: 20 cm (range 10–30 cm)
Diameter: 2.2 mm (range 1.5–3 mm)
The right gastroepiploic artery originates from the gastroduodenal artery. It travels along the greater curvature of the stomach and gives off the four major branches to the omentum, as well as multiple short branches to the stomach – the gastric arteries. It eventually anastomoses with the left gastroepiploic artery.
Minor:
left gastroepiploic artery
Length: 20 cm (range 10–30 cm)
Diameter: 2 mm (range 1.2–2.9 mm)
The left gastroepiploic artery arises from the splenic trunk. It courses along the greater curvature of the stomach and anastomoses with the right gastroepiploic artery.
Venous Drainage of the Flap
Primary:
right gastroepiploic vein
Length: 20 cm (range 10–30 cm)
Diameter: 2.7 mm (range 2–3.4 mm)
The right gastroepiploic vein drains into the superior mesenteric vein. It runs from left to right along the greater curvature of the stomach and parallel to the right gastroepiploic artery. Its caliber is comparable with the size of the artery; however. it is often quite thin and care should be taken while handling it.
Secondary:
left gastroepiploic vein
Length: 20 cm (range 10–30 cm)
Diameter: 2.7 mm (range 2–3.4 mm)
The left gastroepiploic vein runs from the right to the left along the greater curvature of the stomach and parallel to the left gastroepiploic artery. It drains into the splenic vein.
Flap Innervation
Sensory:
none
Motor:
none
Flap Components
The omentum flap can be harvested as a gastro-omental flap by including a patch of the greater curvature of the stomach.
Advantages
- •
Free flap or pedicled flap
- •
Thin and pliable
- •
Large surface area
- •
Long pedicle
- •
Angiogenic and immunogenic properties
- •
Relatively fast and easy harvest
- •
Robust blood supply
Disadvantages
- •
Donor site morbidity may be considerable as it requires laparotomy for access
- •
Size and availability cannot be assessed preoperatively
Preoperative Preparation
Flap Design
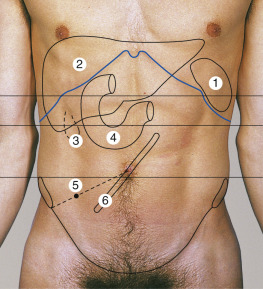
Anatomic Landmarks ( Fig. 36.2 )
General Thoughts About Flap Design
Flap design varies according to defect size. The whole omentum or part thereof can be harvested based on the gastroepiploic vessels and one or more branches of the intra-abdominal arcade. As the flap cannot be combined with a skin paddle, it must be covered with a split-thickness skin graft (STSG) or regional skin flaps.
Special Considerations
- •
Free gastro-omental flap for oral or oropharyngeal reconstructions
- •
Free omentum flap for reconstruction of extensive scalp, lower extremity (consider flow through flap) or head and neck defects
- •
Pedicled omentum flap for chest wall, abdominal wall and breast reconstruction – pedicle can be tunneled subcutaneously or through small diaphragmatic opening
Difference in Design, if Any, When Performing the Flap as Pedicled or Free
No general differences are in the design of flap when using it as pedicled or free. However, the harvesting technique (open vs laparoscopic) and closure of donor site may vary.
Flap Dimensions
Omentum Dimensions
Length: Average 35 cm
Width: Average 25 cm
Thickness: Average 1 cm
The size of the omentum varies significantly with the size of the patient and previous intra-abdominal surgeries or infections. Folding the flap onto itself can increase its thickness.
Flap Markings
Once the omentum is visualized, the area to be harvested is marked. Usually, the entire omentum is harvested.
Patient Positioning
Supine positioning of patient for harvest. Repositioning after flap harvest may be necessary according to site of defect.
Anesthetic Considerations
General anesthesia.
Technique of Flap Harvest ( Figs 36.6 , 36.7 )
An upper median laparotomy is performed. The abdominal cavity is explored and the omentum is inspected for surface area, volume, and pedicle length. It is elevated off the transverse colon and is mobilized on the gastroepiploic arcade. This dissection is performed in a thin areolar and avascular plane using blunt dissection and needle-tip cautery to ensure bloodless dissection. The lateral splenic attachments are divided as well as the short gastric vessels to free the omentum from the greater curvature of the stomach. The flap is based on the right or left gastroepiploic artery; the contralateral vessels are ligated. Care is taken to prevent kinking or twisting of the pedicle when transposing the flap into the chest wall defect.
Laparoscopic Harvest
Standard laparoscopic surgery techniques are used with four ports placed in the umbilical region, suprapubic region, and both lateral iliac fossa. CO 2 pneumoperitoneum of 10–12 mmHg is maintained during the procedure. The gastric wall is elevated and the right gastroepiploic artery is isolated. The short gastric arteries along the greater curvature are ligated until the left gastroepiploic artery is reached. The omentum is carefully released from the transverse colon preserving the mesocolon vascularity. The left gastroepiploic artery is ligated adjacent to the left colic flexure and the flap is evacuated through one of the ports.
Flap Modification/Flap Handling
As the gastroepiploic arteries give off several short branches to the greater curvature of the stomach, a patch of gastric mucosa can be included in the flap for oral or oropharyngeal reconstructions.
Special Instruments
Laparoscopic harvest can considerably reduce the donor site morbidity.
Donor Site Closure and Management
After harvesting the omentum as a free flap, standard laparotomy or laparoscopy closure techniques are used.
When the omentum is harvested as a pedicled flap, a small defect must remain in the abdominal fascia to permit passage of the pedicle. This, by definition, creates an abdominal hernia. However, as long as it is not symptomatic it will not require intervention. Sutures are placed between the greater curvature of the stomach and the transverse mesocolon to minimize the chance of volvulus.
A drain is not usually necessary at the donor site.
Technical Tips to Optimize Outcomes and Avoid Complications
Relative contraindications for the use of the omental flap are previous multiple intra-abdominal surgeries or previous intra-abdominal infections (peritonitis). If the decision is made to proceed, extra care should be taken to avoid injury.
The flap can be lengthened considerably by dividing the gastroepiploic artery between the right and the left omental artery. Vascularization of the entire flap is provided by the anastomoses between the left, right, and middle omental artery within the intra-abdominal arcades.
Flap Usage
Typical Indications for the Use of This Flap
Pedicled (see Cases 36.1, 36.2 )
Reconstruction of extensive chest wall or sternal defects: the omentum can be transposed into the chest wall or sternal defect through a hole in the diaphragm or a fascial defect in the abdominal wall. The flap is covered with a STSG or local skin flaps. The arc of rotation of the flap reaches most defects on the chest and abdominal wall.
Free Flap
- •
Reconstruction of extensive scalp or lower extremity defects, chronic avascular or irradiated wounds
- •
For lower extremity reconstructions flow through flap designs can be considered to ensure perfusion of distal part of the limb
Atypical Indications for the Use of This Flap
Pedicled
Reconstruction of the breast in Poland syndrome or implant coverage after mastectomy. Use laparoscopic technique whenever possible (see above). After ligation of left gastroepiploic artery, a small incision is made in the inframammary fold and a small subcutaneous tunnel is created up to the subcostal margin. The fascia and peritoneum are incised in the midline. The flap is pulled through the fascial gap, tunneled subcutaneously, and placed in the defect.
Free Flap
Head and neck reconstruction with gastro-omental composite free flap. The short gastric arteries are left intact while the left gastroepiploic vessels are ligated. The gastric patch is excised using a gastrointestinal stapling device taking care to avoid pyloric outlet.
Postoperative Care
General
Avoid heavy weight-lifting for 6–8 weeks.
Recipient Site
General wound and flap care. If STSG had been used for flap coverage, first dressing change is done on POD 5.
Donor Site
An abdominal binder may be recommended for 4 weeks, no heavy weightbearing for 4 weeks. After pedicled omentum flaps a considerable abdominal wall hernia can develop. Although it may be cosmetically unsightly, it can be neglected as long as it is not symptomatic.
Outcomes
Expected Outcomes
The omentum flap provides versatile, thin, pliable coverage for various defects and recipient sites. It has a robust blood supply as well as high angiogenic and immunogenic potential. It is most beneficial in defects with a large surface area, chronic avascular or irradiated wounds, or wounds with a high bacterial load.
If the flap can be harvested laparoscopically, the donor site is quite appealing and complications as abdominal wall hernias can be avoided. Pedicled flaps create an abdominal wall hernia by definition, as the pedicle has to be guided through a fascial gap but as long as they are asymptomatic no treatment is needed.
Untoward Outcomes
Large abdominal wall hernias can develop after pedicled omentum flaps. Additionally, all intra-abdominal procedures may result in adhesions of varying extent. Gravitational forces may cause sagging of the flap, especially in head and neck reconstructions. When using a gastro-omental flap for reconstruction of the oral cavity, extensive mucus and acid production may be troublesome. Spontaneous flap growth has been described after transposition.
Superior Epigastric Flap
Flap Anatomy (see Fig 11.2 , Fig 11.3 , Fig 11.8 , Fig 11.9 )
Arterial and Venous Supply of the Flap (see Figs 11.2 and 11.3 )
The blood supply to the superior epigastric flap is provided by perforators of the superior epigastric artery (SEA) The SEA originates together with the musculophrenic artery from the internal mammary artery at the sixth intercostal cartilage. It passes behind the seventh costal cartilage, perforates the posterior rectus fascia, and enters the rectus abdominis muscle at a variable distance. After giving rise to the superficial SEA, a large musculocutaneous perforator that travels subcutaneously along the costal margin, the SEA gives off several perforators to the overlying skin. On average, 4–5 perforators can be found on the upper hemi-abdomen, most of them encountered in an area 2–6 cm from the midline and 0–10 cm below the xiphoid process. The diameter of the perforators is on average 0.82 mm and they are accompanied by a minimum of one vein. Location and number of perforators may vary significantly between individuals.
Dominant:
superior epigastric artery perforators
Length: 3.4 cm (range 1.5–7 cm)
Diameter: 0.8 mm (range 0.5–2 mm)
Venous Drainage of the Flap ( Fig. 11.8 )
Primary:
superior epigastric perforating veins
Length: 3.4 cm (range 1.5–7 cm)
Diameter: 0.8 mm (range 0.5–2 mm)
Flap Innervation ( Fig. 11.9 )
Innervation to the skin of this flap is through anterior and lateral cutaneous branches of intercostal nerves 5–9. However, the flap is usually planned as an islanded flap and therefore not innervated.
Flap Components
The superior epigastric flap is a fasciocutaneous perforator flap. Anterior rectus fascia can be harvested with the flap although this would weaken the abdominal wall.
Advantages
- •
Less invasive, no use of muscle
- •
Primary closure of donor site
- •
Relatively fast and easy harvest
Disadvantages
- •
Limited mobility
- •
Perforator anatomy may be variable
Preoperative Preparation
Flap Design
Anatomic Landmarks
- •
Caudal: midpoint between xiphoid and umbilicus
- •
Cranial: xiphoid
- •
Lateral: anterior axillary line
- •
Medial: midline
General Thoughts About Flap Design
The vascular territory of the superior epigastric artery and the corresponding perforasomes have been studied extensively. Flap design in a horizontal direction yields better outcome than in a vertical direction and can be harvested as far as the anterior axillary line. The donor site can be closed primarily with a reversed abdominoplasty procedure.
Special Considerations
The superior epigastric flap is most useful as a propeller-style perforator flap for chest wall, sternal or breast reconstructions. The flap can be raised and transferred as an island flap or with a small cutaneous bridge left intact and rotated up to 90° into the defect. Unlike other perforator flaps, it is not necessary to completely skeletonize the perforator.
Difference in Design, if Any, When Performing the Flap as Pedicled or Free
The superior epigastric flap is mostly used as pedicled perforator flap.
Flap Dimensions
Skin Island Dimensions
Length: average 25 cm (range 16–38 cm)
Width: average 9 cm (range 6–15 cm). Maximum to close primarily depends on skin laxity
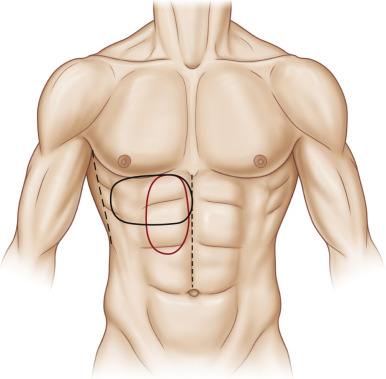
Flap Markings ( Fig. 36.3 )
The flap is marked on the skin overlying the perforators of the superior epigastric artery. The flap is marked in the horizontal or vertical direction, with the horizontal design being preferable.
Patient Positioning
Supine positioning of the patient.
Anesthetic Considerations
General anesthesia.
Technique of Flap Harvest
The superior epigastric artery perforators are identified using a handheld Doppler. The flap is designed horizontally, with the most suitable perforator as the pivot point. The fasciocutaneous flap is elevated in a lateral to medial direction in the suprafascial plane until the perforator has been identified. The perforator is dissected sufficiently to guarantee unrestricted transposition of the flap into the defect.
Flap Modification/Flap Handling
Vascular territories of the superior epigastric artery lie between the midline and the anterior axillary line and the xiphoid and the midpoint between the xiphoid and the umbilicus. To avoid necrosis of the distal tip flap designs should not reach beyond those borders unless the flap is delayed. As the vascular anatomy may be quite variable, perforators should be marked preoperatively using a hand-held Doppler. The flap is raised in a lateral to medial direction or, if a vertical flap design is preferred, in a caudal to cranial direction in the suprafascial plane.
Special Instruments
Handheld Doppler
Donor Site Closure and Management
The donor site can usually be closed primarily using a reversed abdominoplasty technique. Frequently the scar can be concealed in the inframammary fold. At least one drain should be placed subcutaneously at the donor site and under the flap.
Technical Tips to Optimize Outcomes and Avoid Complications
Further pedicle length can be achieved by dissecting the perforator to the SEA and transecting the SEA distal to the perforator takeoff. This would require an intramuscular dissection of the perforator. The pedicle length is increased and the arc of rotation can be much wider.
Flap Usage
Typical Indications for the Use of This Flap
Pedicled
Reconstruction of chest wall, sternal, or breast defects.
Postoperative Care
General
- •
Care is taken to avoid compression anywhere around the flap and the pedicle of the flap.
- •
Flap monitoring is performed on a regular basis.
- •
The patient is positioned in a way to avoid tension of the flap, head of bed slightly elevated.
- •
Avoid heavy weight-lifting for 6–8 weeks
Recipient Site
To avoid tension on wound edges patients with larger breasts should wear a bra 24 h/day until complete wound healing has been achieved.
Donor Site
General wound care, avoid heavy weight-lifting for 6–8 weeks. Abdominal binder may be recommended in the first 4–6 weeks postoperatively if extensive undermining for reversed abdominoplasty was necessary.
Outcomes
Expected Outcomes
The superior epigastric flap provides adequate coverage for chest wall, sternal, and certain types of breast reconstruction. The donor site is very inconspicuous if the scar can be concealed in the inframammary fold.
Untoward Outcomes
In sternal reconstructions meticulous debridement of the infected bone has to be performed prior to reconstruction to avoid persistent osteomyelitis with consequent osteocutaneous fistula or flap failure. Distal tip necrosis may occur if the flap was designed beyond the borders of the vascular territories.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


