Omental Flap for Thoracic Reconstruction
Amir Inbal
David H. Song
DEFINITION
The omentum is rich in vasculature, lymphatics, and fat and serves an important immunologic function within the abdominal cavity.
The original anatomical term epiploic is derived from the Greek word epipleein, which means to float on. It was so named to reflect how the omentum “floated” anterior to the intestines.
The omental flap can be harvested as a pedicled or free flap and is commonly used as a pedicled flap for thoracic reconstruction.
These flaps are historically used to revascularize the myocardium and cover intra-aortic balloon pumps and ventricular assist devices.
Thoracic and chest well defects are attributable to congenital malformations or acquired deformities and can cause significant physical and psychological morbidity.
ANATOMY
The region of the thorax amenable to pedicled omental flap reconstruction includes the central and lateral thorax and its contents, most commonly the sternum, pericardium, pleural cavity, and at times the overlying skin. When needed, the flap can extend to reach beyond the chest.
Thorax: Composed of the skin, muscles, bones, and internal organs/structures located between the neck and the abdomen
Muscles include pectoralis major, pectoralis minor, serratus anterior, serratus posterior, rectus abdominis, external oblique, intercostal muscles, latissimus dorsi, and trapezius.
Thoracic skeleton
Ribs—form the rib cage by attaching to vertebral bodies posteriorly and sternum anteriorly (variable)
Sternum—long, flat bone in the center of the chest composed of the manubrium, body, and xiphoid process
Thoracic vertebrae
Internal organs/structures that should be addressed when reconstructing the thorax include the lungs, heart, pericardium, pleura and pleural space, esophagus, trachea and bronchus, superior vena cava, thymus gland, diaphragm, liver, gallbladder, pancreas, duodenum, and pancreas.
Dominant blood supply provided by paired internal mammary arteries (branch of subclavian artery)
Run posterior to costal cartilage adjacent to sternum with one or two venae comitantes.
Interconnect with transverse cervical, thoracoacromial, lateral thoracic, and posterior intercostal arteries.
Cutaneous perforating vessels supply overlying tissues and skin
Omentum
The omental flap is based on the greater omentum found in the abdominal cavity (FIG 1A).
It contains visceral peritoneum, fat, lymphatic tissue, a rich vascular arcade, and macrophage collections (milky spots).
It is a nonneurotized flap.
It originates from the peritoneum of the greater curvature of the stomach. From here, the two layers of the visceral peritoneum descend anterior to the small intestines, folding backward upon itself at a variable level within the abdominal or pelvic cavity to ascend and enclose the transverse colon before attaching to the posterior abdominal wall. With the two layers of visceral peritoneum folded upon itself, it effectively creates a four-layered structure.
The right border of the greater omentum may be attached to the second portion of the duodenum.
The left border of the greater omentum is continuous with the gastrosplenic ligament.
In a study of 200 cadavers and 100 patients who had abdominal surgery, the average omental length was 25 cm for men (range, 14-36 cm) and 24 cm for women (range, 14- 34 cm). The average omental width was 35 cm for men (range, 23-46 cm) and 33 cm for women (range, 20-46 cm). Size of the omental flap ranges from 300 to 1500 cm2.1
The greater omentum is supplied by the right and left gastroepiploic arteries, which communicate with a rich vascular network within the two layers of the greater omentum along the greater curve of the stomach (FIG 1B).
Vascular supply from the right: celiac trunk to common hepatic artery to gastroduodenal artery to right gastroepiploic artery
Vascular supply from the left: celiac trunk to splenic artery to left gastroepiploic artery
The short gastric arteries originating from the splenic artery, superior to the left gastroepiploic artery, also serve as an additional source of blood supply to the omentum by multiple collateral vessels.
The right gastroepiploic artery is usually the dominant vessel supplying the omentum. It is usually 2 to 3 mm in size, and the vein is typically larger.
From the anastomoses of the right and left gastroepiploic arteries, the accessory, right, middle, and left omental arteries descend within the greater omentum. There is a rich connective arcade between these vessels within the omentum.
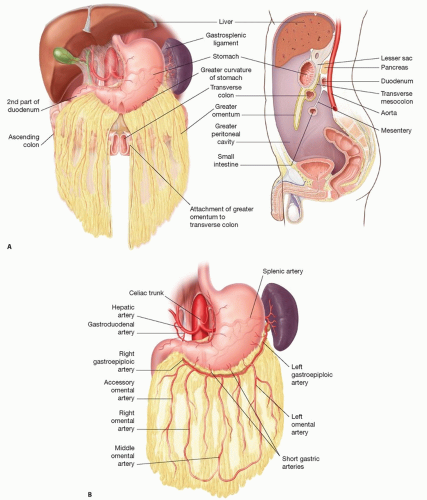
FIG 1 • A. Anatomy of the greater omentum within the abdominal cavity. B. Vascular anatomy of the omental flap.
Type 1 (81.7%): middle omental artery bifurcation in the lower third, with anastomoses to the right and left omental arteries
Type 2 (11.0%): middle omental artery bifurcation in the middle third, before anastomoses to the terminal branches of the right and left omental arteries
Type 3 (4.5%): middle omental artery bifurcation in the upper third into two or three branches
Type 4 (1.2%): middle omental artery absent and replaced by several short omental arteries
Type 5 (1.6%): Left omental artery does not join the left gastroepiploic artery
A robust venous system accompanies the arterial arcade and drains into the right and left gastroepiploic veins.
PATHOGENESIS
Full-thickness defects of the anterior thoracic cavity can arise from a variety of causes:4
Infections
Necrotizing soft tissue infections
Mediastinitis
Sternal osteomyelitis
Fistulae
Bronchopleural
Esophagopleural
Trauma
Iatrogenic
Radiation injury
Postsurgical wound breakdown
Exposed hardware (eg, aortic grafts, breast implants, vertebral, sternal plates, or ventricular assist devices)
Neoplastic
Contour congenital defects of the chest wall
Poland syndrome
Other breast defects
Flail chest: paradoxical chest movement during respiration of a portion of the rib cage after it loses continuity with the surrounding chest wall resulting in inefficient ventilation.
Most often the result of trauma or oncologic resection of a significant portion of the chest wall
May require reconstruction with soft and/or bony tissue
Defects 5 cm in diameter or larger generally require skeletal fixation.
Risk factors for sternal dehiscence and infection include chronic obstructive pulmonary disease, obesity, diabetes, and bilateral harvest of the internal mammary vessels.
Radiation-induced injury may cause significant scarring and nonfunctional tissue that will require debridement and reconstruction.
NATURAL HISTORY
Without adequate treatment, defects of the anterior thorax can lead to devastating consequences including paradoxical breathing, osteomyelitis, mediastinitis, and death.
The greater omentum can be harvested from the abdominal cavity without any major loss of function.
Over time, the omental flap contracts slightly to “bed down” at the defect site.
The omental flap provides soft tissue coverage only. In cases in which the chest wall is unstable due to loss of structural support, alternative methods such as wires, plates, mesh, or bony reconstruction are required.
PATIENT HISTORY AND PHYSICAL FINDINGS
The preoperative evaluation for patients requiring thoracic reconstruction includes a detailed assessment of the etiology of the defect, the patient’s underlying medical and functional status, the state of the pleural cavity, the extent of the soft tissue defect, and whether skeletal support is required and reconstructive options available.
It is important to note whether the internal mammary vessels have been previously injured or sacrificed.
The etiologic factors of the defect should be elicited in history taking, as well as its suitability for reconstruction.
Dirty or actively infected wounds or those with residual tumor are not amenable to reconstruction.
Bacterial cultures should be obtained and targeted antibiotic therapy started as necessary.
A detailed medical history should be noted including cardiovascular problems, lung pathology, smoking, immunocompromise, and nutritional status.
As much as possible, any underlying medical condition should be corrected or optimized prior to undergoing definitive reconstruction.
Special attention should be addressed with regard to history of previous abdominal surgery, trauma, and any other abdominal morbidity, as these may cause to preclude the omentum flap as a reconstructive option.
Available reconstructive options or prior attempts at reconstruction should be noted.
Physical examination
The skin is inspected for previous scarring, prior incisions, active infection, or radiation changes.
Hernias are noted. Laparoscopic surgical port site scars should be carefully searched. Any prior surgery in the abdominal cavity can lead to intra-abdominal adhesions, increasing the difficulty of omental flap harvest.
Missing tissues are noted.
Soft and/or hard tissue defects may be present.
Breathing mechanics are evaluated.
Pulmonary function tests are useful for evaluation of baseline pulmonary status.
Routine preoperative laboratory testing should be performed.
Obtain a baseline chest radiograph.
Computed tomography (CT) should be considered in cases of complex or extensive defects.
The defect should be thoroughly examined again, if possible, under general anesthesia. The location, size, depth, and extent of the defect must be noted. Exposed vital structures such as the pericardium, major vessels, or hardware require more emergent coverage. Active infection or tumor should be excluded.
Patients may present with postoperative sternal wounds after cardiac or mediastinal surgery.
Pairolero and Arnold classified wounds based on timing of presentation of infection:4
Type I—Occur soon after surgery, may contain incisional breakdown with serosanguineous discharge and/or sternal instability
Type II—Occur weeks after surgery, and cellulitis, mediastinal purulence, and positive cultures may be present
Type III—Occur months to years after surgery and contain draining sinus tracts and chronic osteomyelitis
Type II and III wounds often require operative reconstruction.
IMAGING
Thoracic imaging
Chest radiographs in the anteroposterior and lateral dimensions can aid in assessment of the defect. Although lacking in sensitivity and specificity, they can be helpful in raising suspicions for other cardiac or lung pathology.
CT scans of the thorax are useful in preoperative evaluation of the thoracic structures, in delineating the extent of the defect, as well as in locating any underlying tumor or abscess.
Compared with CT scans, magnetic resonance imaging (MRI) scans are more sensitive at detecting osteomyelitis and evaluating the soft tissues. However, they are seldom required.
Vascular studies such as CT angiography may be warranted if tumor resection or trauma is thought to compromise the vascular anatomy or when extent of vascular involvement is unknown. In addition, if a free flap is planned, the vasculature anatomy can be assessed for recipient vessels.
Abdominal imaging
In general, no investigations are needed to assess the omentum. In cases of previous abdominal surgery or trauma, where there may be significant adhesions or damage to the omentum, use of the omental flap would be avoided. An exception is previous laparoscopic surgery where no complications and minimal manipulation of abdominal contents have been confirmed.
CT of the abdominal wall may assist in evaluating patients with a history of surgery or trauma to the area.
Vascular studies such as CT angiography may be warranted if compromised vascular anatomy is suspected secondary to previous surgery or trauma.
Laparoscopic surgery enables a direct intraoperative “peak” at the omentum and its vascularity facilitating decision-making regarding its use.
DIFFERENTIAL DIAGNOSIS
Other flaps that can be used to reconstruct defects of the anterior thoracic cavity include:
Pedicled flaps
Pectoralis major muscle flaps
Advancement based on the thoracoacromial blood supply
Turnover based on the internal mammary blood supply
Rectus abdominis flaps based on the superior epigastric artery
Muscle only
Myocutaneous
Latissimus dorsi flaps (usually for more lateral defects of the anterior thoracic cavity)
Internal mammary artery perforator flap
Free flaps
NONOPERATIVE MANAGEMENT
When left long enough, any wound can heal without operative intervention. However, healing time, exposure of vital mediastinal structures or hardware, and the risk of intervening infection must be taken into consideration.
There are a variety of wound dressings that can be used, ranging from simple wet-to-dry dressings to advanced silver-containing biomaterials, which are beyond the scope of this chapter.
A useful bridge to reconstruction is the use of a negative pressure wound therapy (NPWT) system, which can aid in wound bed preparation and allow for patient and wound optimization prior to definitive wound coverage.
SURGICAL MANAGEMENT
Preoperative Planning
The omental flap can be harvested as a pedicled or free flap. For defects of the thorax, it is commonly used as a pedicled flap.
The size of the omental flap is variable and dependent on individual patient anatomy.1 The reach of the pedicled omental flap depends on its size.
Compared with muscle flaps, omental flaps allow better lining of the inferior third of the mediastinum, provide more bulk, and conform to the deep recesses of the mediastinum.5
The general indications for the use of thoracic defects requiring omental flap reconstruction are6:
Full thickness in nature exposing the underlying bone, mesh (eg, ADM), hardware, or mediastinal contents
Where dead space obliteration in the thorax is required
Considered a good option for radionecrotic chest wounds, with its theoretical advantage of having immunogenic properties.
Foul-smelling, contaminated, or infected wounds
Provides a large surface area cover especially when extending the arc of rotation. If used for skin and subcutaneous tissue coverage, the omental flap can be skin grafted in the same sitting.
When covering a prosthetic material, musculocutaneous flaps are preferred to omentum and skin graft owing to a better seal by the former.
Good source of bulk providing volume for pleural defects or any dead space obliterationRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree