Preoperative setting: the patient lies prone with the head in neutral position over a prone pillow so that he/she can place the arms underneath it, allowing the surgeon to have a closer and better view of the operating field. Then, the inion has to be identified, which is the most prominent and highest point of the external occipital protuberance. It lays at the middle of the superior nuchal line, thus indicating the middle sagittal plane. It is of paramount importance to identify the inion since it guides the preoperative marking: two incision lines, one at each side of the inion, need to be drawn along the superior nuchal line, which is where the nuchal ligament and the trapezius muscle attach

Prone pillow, specifically designed for surgical procedures on the occipital region

Vessel localization by handheld Doppler: the most important step of the migraine headache deactivation surgery is to precisely identify the trigger point preoperatively. Each extra minute spent at this point is worth it since it will not only reduce the operative time but will also improve greatly the success rate. Therefore, with the patients in prone position, it is asked to precisely identify the points where he/she perceive that migraine attacks start. Then a handheld Doppler examination is performed to confirm the presence of arterial signal at the point indicated by the patient or nearby it. In case of positive Doppler signal, it usually correlates with an ectatic occipital artery closely related to occipital nerves. This point is also marked as it is where most of the surgery would be focused

Operative setting: we commonly perform the surgery with a team of three surgeons, two at each side of the patient’s head that operate independently, with the third on top to help both. We believe that this type of surgery could not be performed without the help of magnification loupes (at least ×3 magnification, ×4.5 better)

Local infiltration of anesthetic solution: now that everything is set, local anesthetic administration can be performed. We usually employ a 40-cc Carbocaine 1% + 40-cc NaCl 0.9% + 20-cc sodium bicarbonate 8.4% solution that not only provides anesthesia but also hydro-dissects tissue planes to facilitate surgical procedure and helps performing trichophytic skin incision

Single central incision: we started our experience in migraine headache deactivation surgery performing a single central incision of 8–10 cm in length along the superior nuchal line. The trichophytic skin incision (parallel to the hair bulbs) was performed (with a no. 20 blade) in order to hide the resulting scar. Accurate hemostasis was performed taking care not to damage hair bulbs in the subcutaneous tissue. In case of diffuse bleeding, 60-s local compression with sterile gauze soaked into a H2O2 solution was usually helpful. Dissection was taken deep by blunt-tip Metzenbaum scissors until both the trapezium and occipitalis muscles’ fascia are exposed. During this step, at least two subcutaneous arteries can be identified and safely coagulated

Double incisions: nowadays, we rather perform two lateral 4 cm incisions centered on the trigger points along the superior nuchal line when patients suffer from bilateral occipital migraine headache

Single lateral incision: we usually performed a slightly longer single 6 cm lateral incision centered on the trigger point along the superior nuchal line when patients suffer from monolateral occipital migraine headache
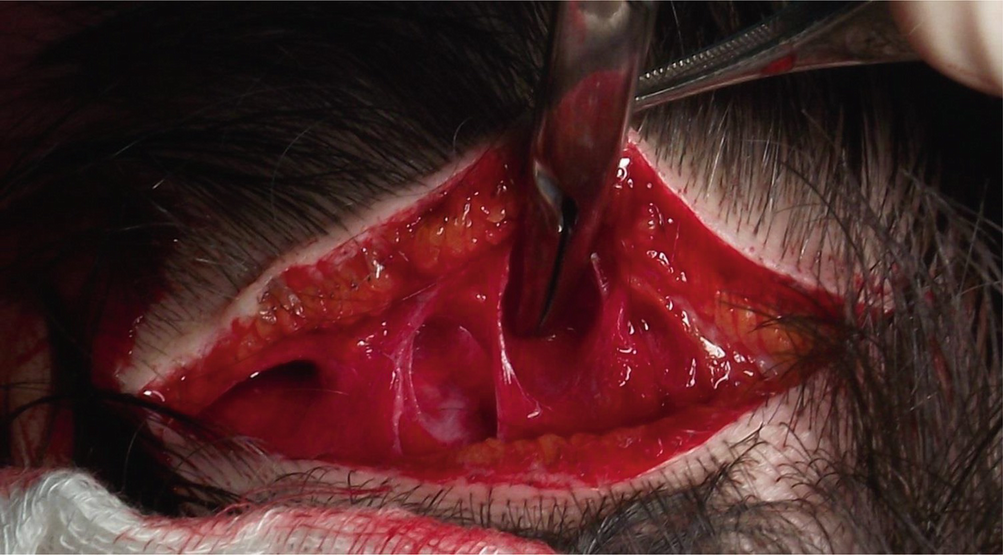
Careful dissection of the occipitalis, trapezius, and splenius muscles is performed again with blunt-tipped scissors perpendicular to the trigger point in order to isolate the occipital nerves and arteries. Once these structures are encountered, the dissection is evenly taken deep to the same portion along all the incision
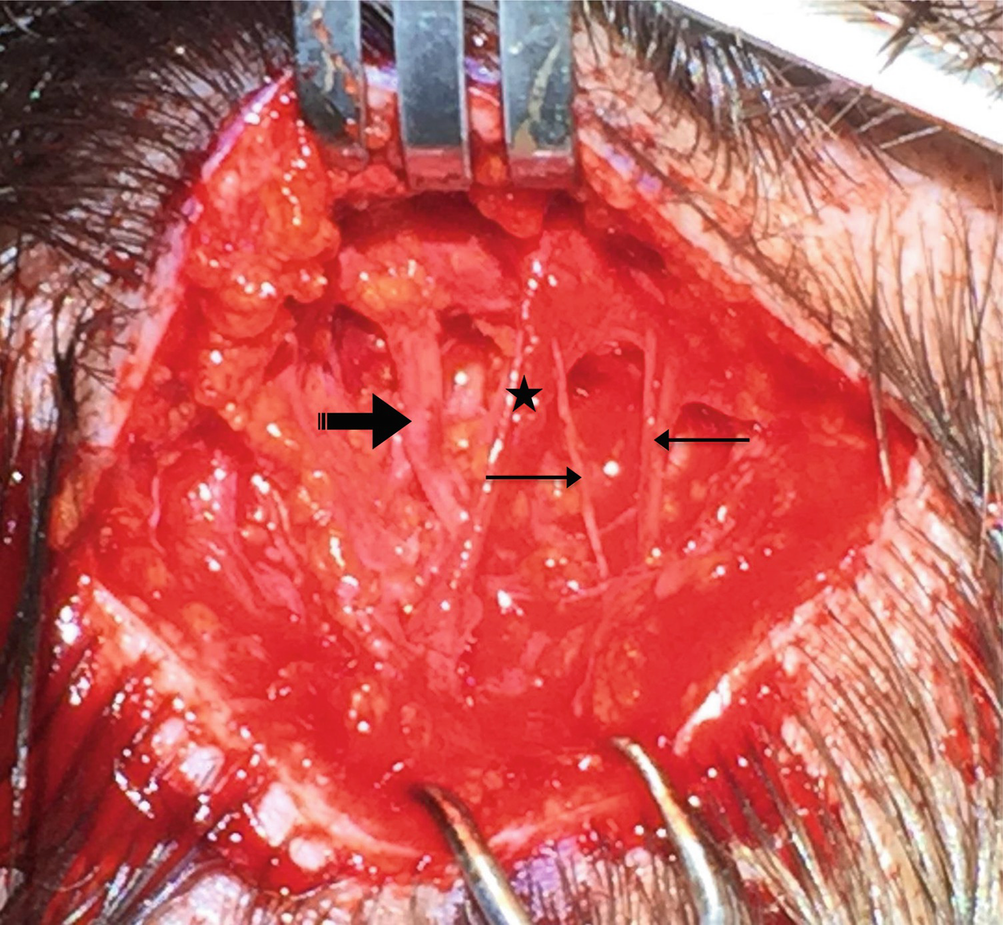
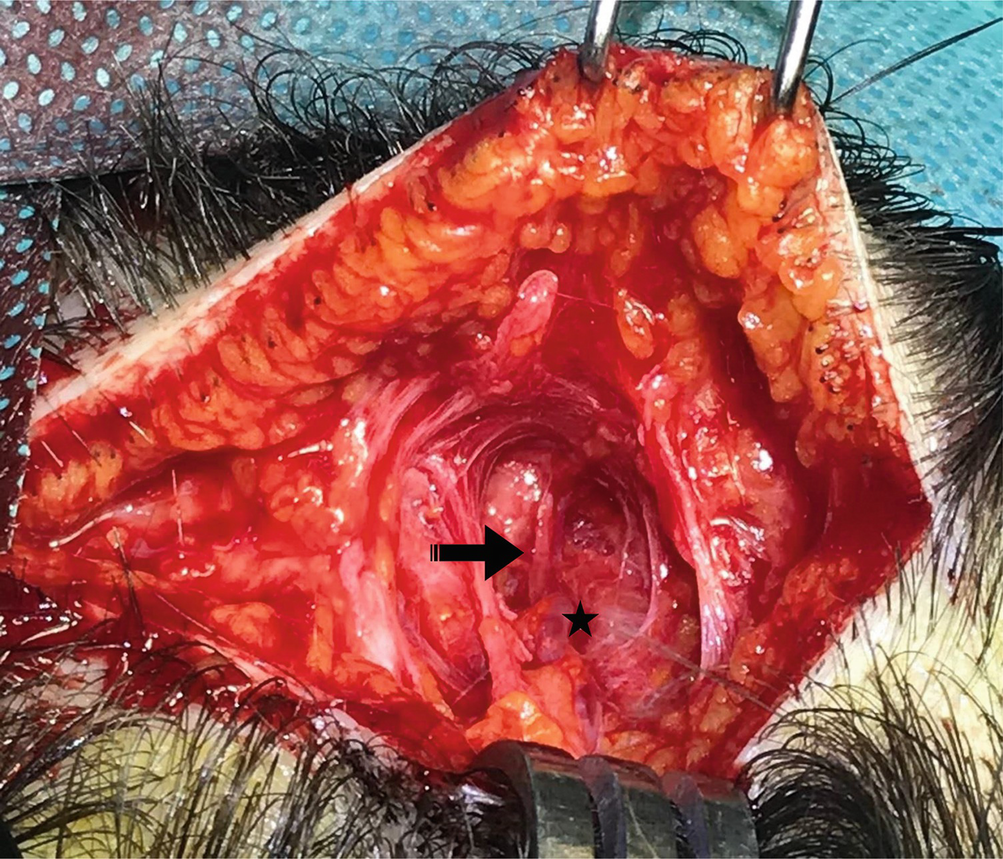
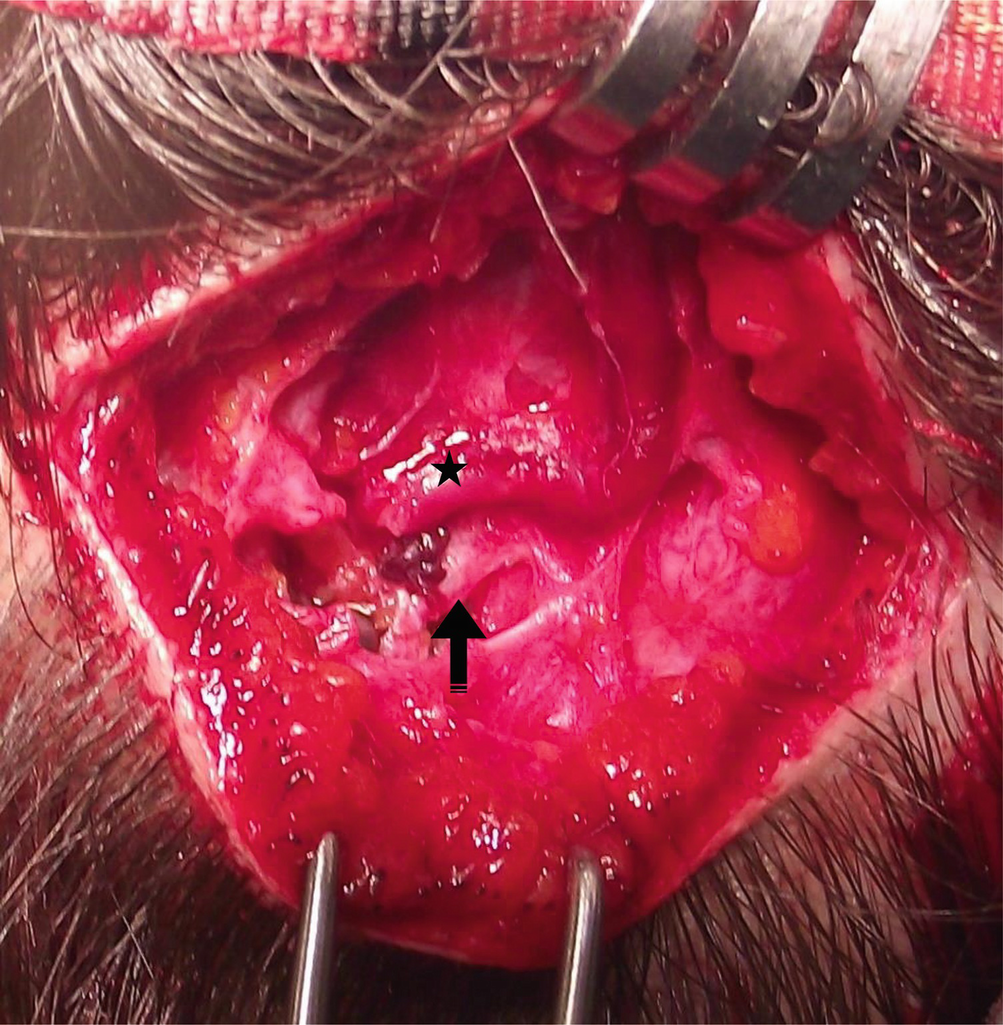
Different intraoperative findings are usually found, and no case is the same as another. Normal occipital artery (star) crossing above the occipital nerve (heavy arrow). At the same surgical plane, branches of the lesser occipital nerve are also usually identified (light arrow)
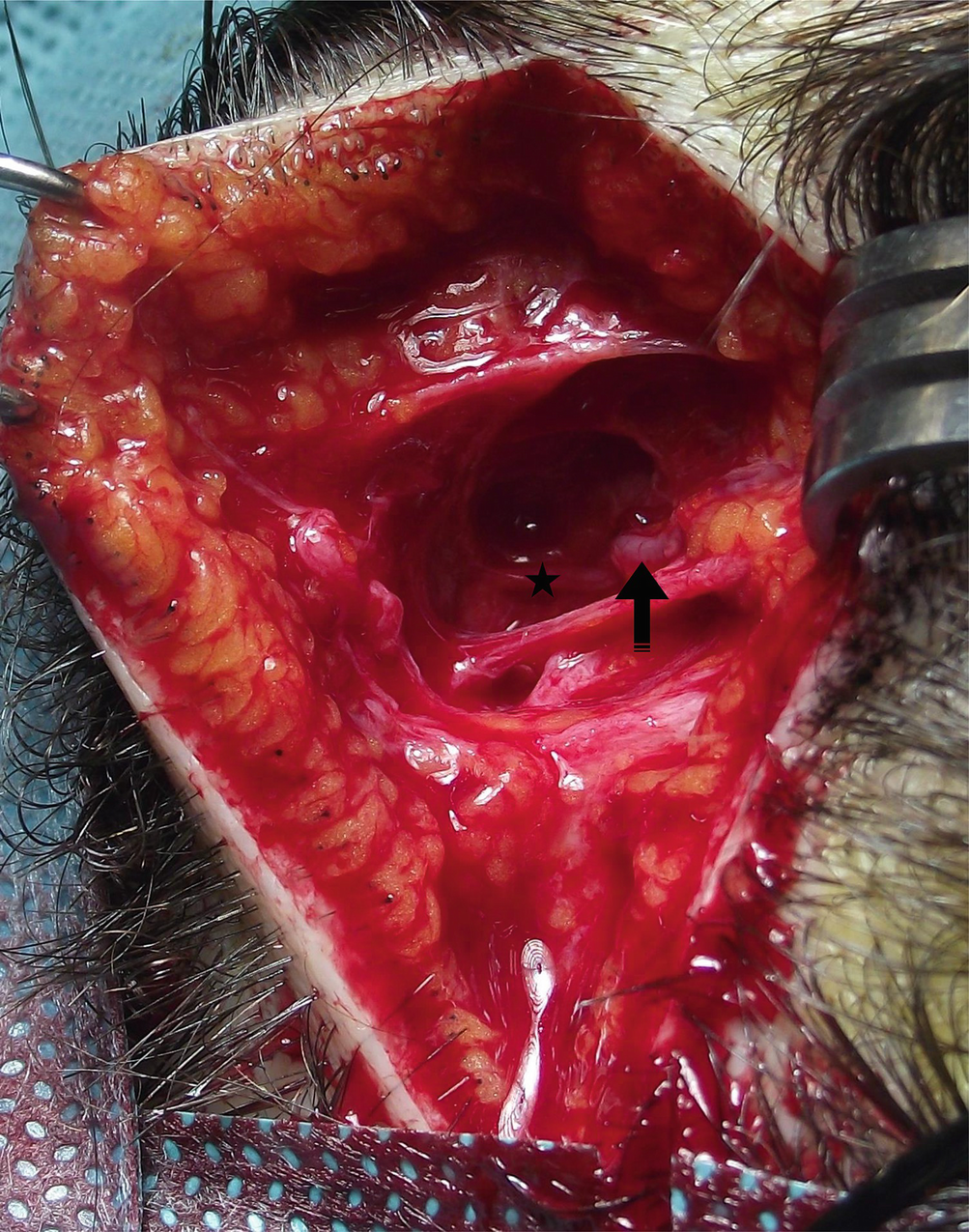
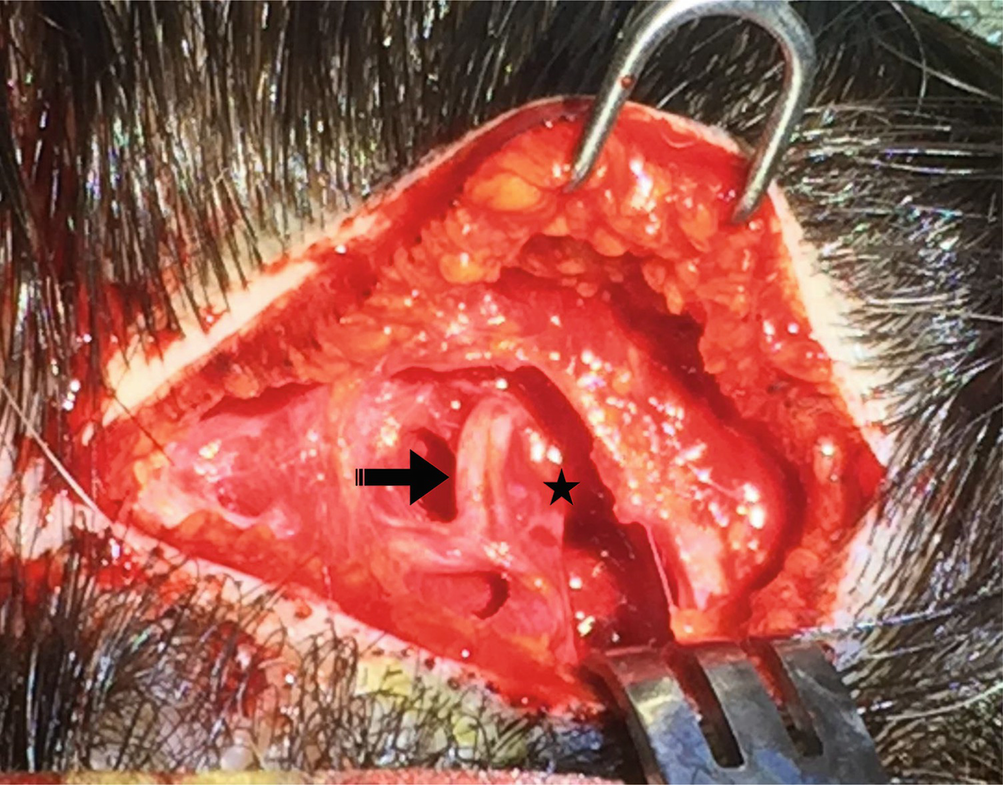
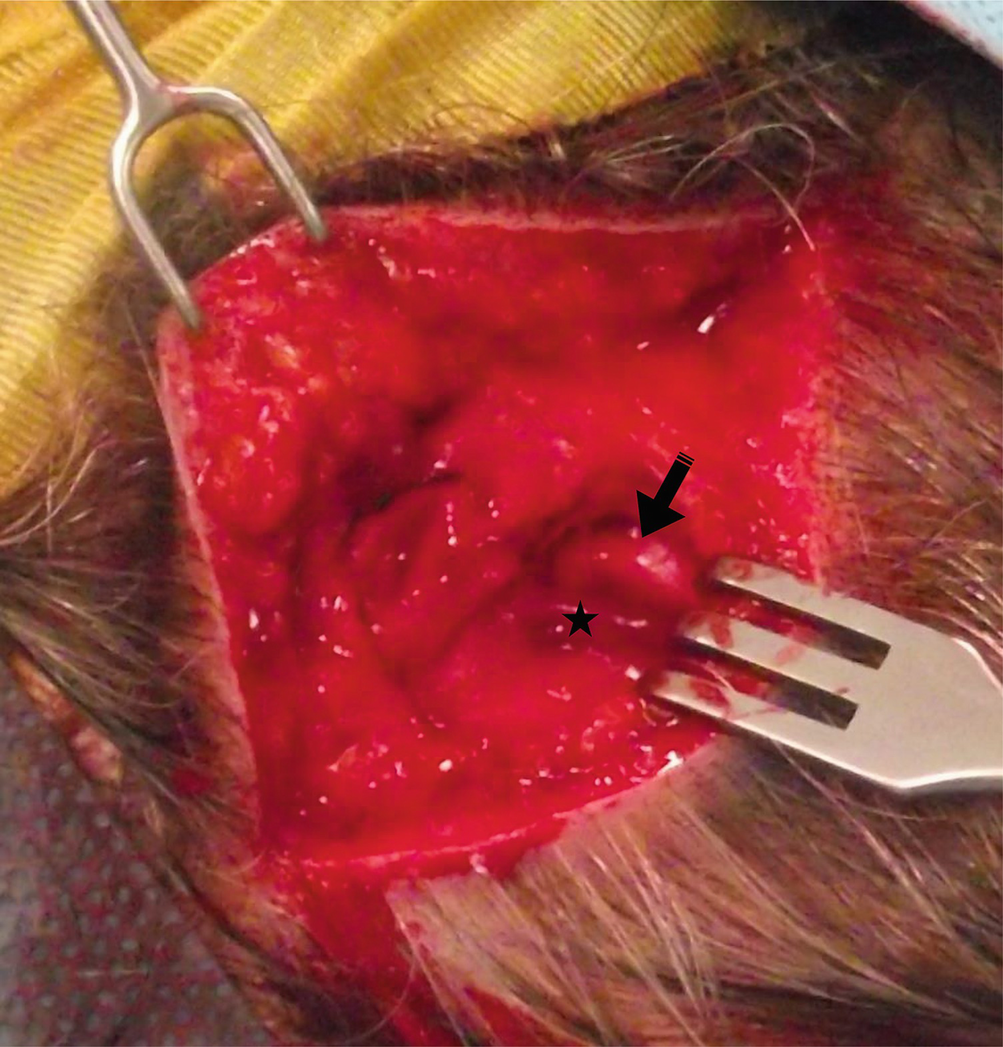
Normal occipital artery (arrow) crossing above the occipital nerve (star)
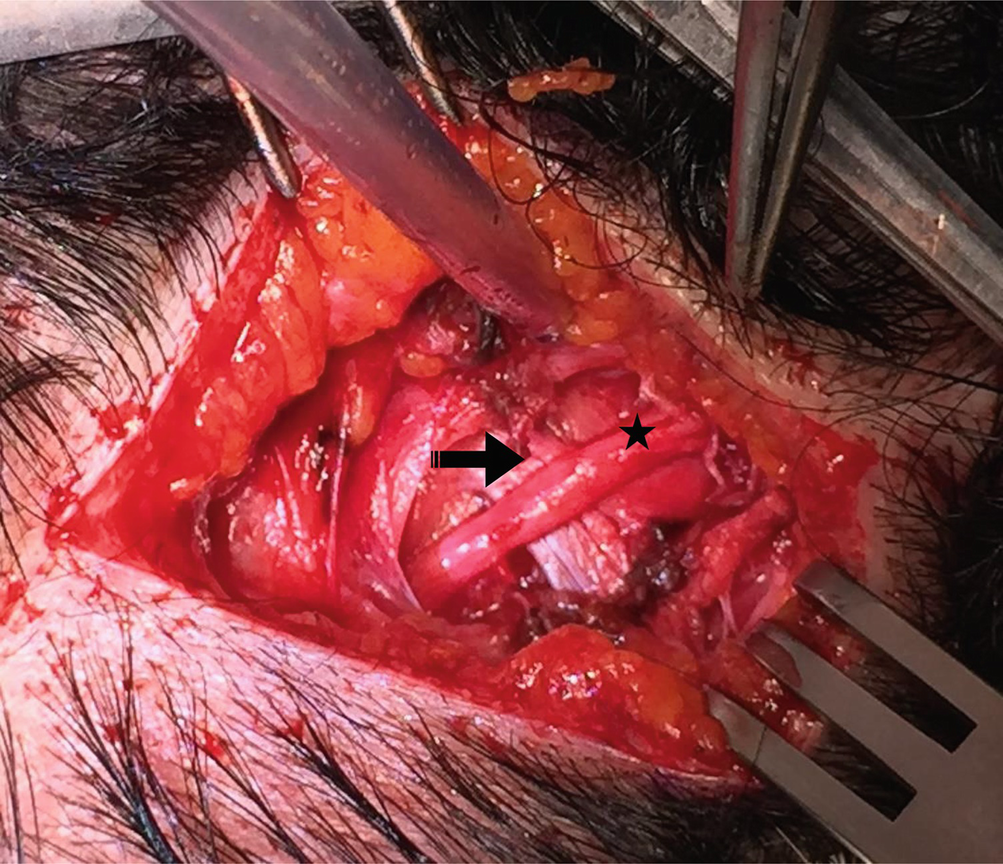
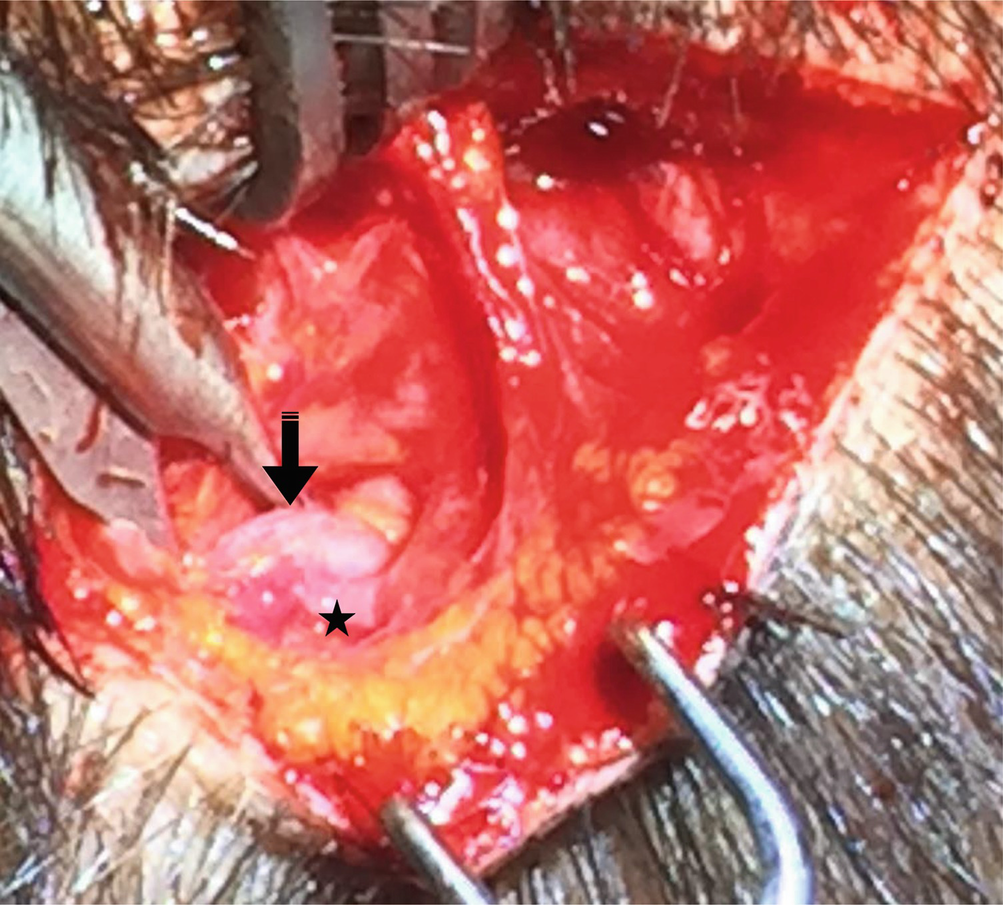
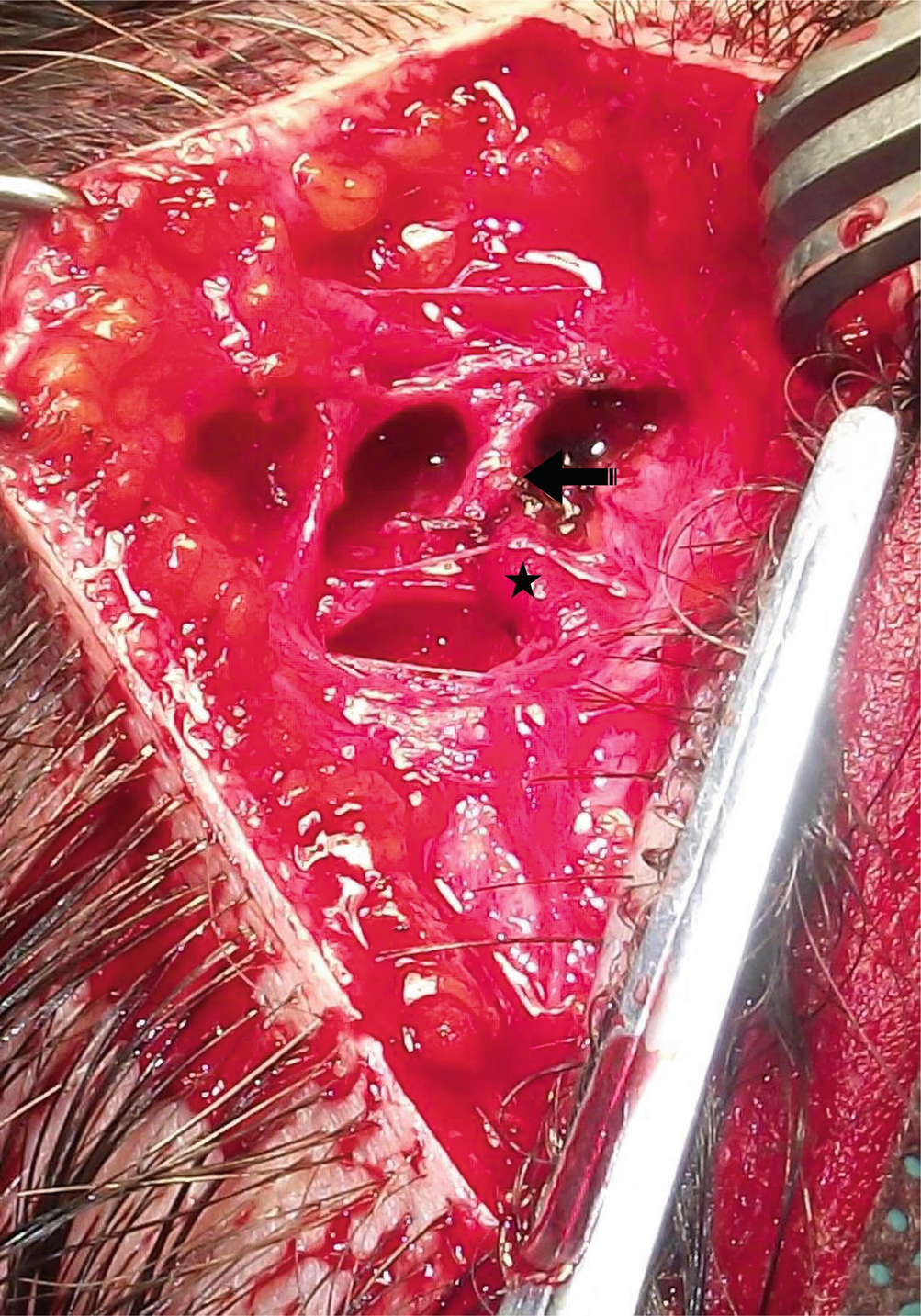
Dilated occipital artery (star) crossing above the occipital nerve (arrow), which appears compressed into an hourglass shape as a consequence of the lasting traumatism
Occipital artery (star) lateral to the greater occipital nerve (arrow) that again appears compressed
Dilated occipital artery (star) running lateral and in strict connection with the occipital nerve (arrow)
Ectatic occipital artery (star) running caudally and laterally to the occipital nerve (arrow)
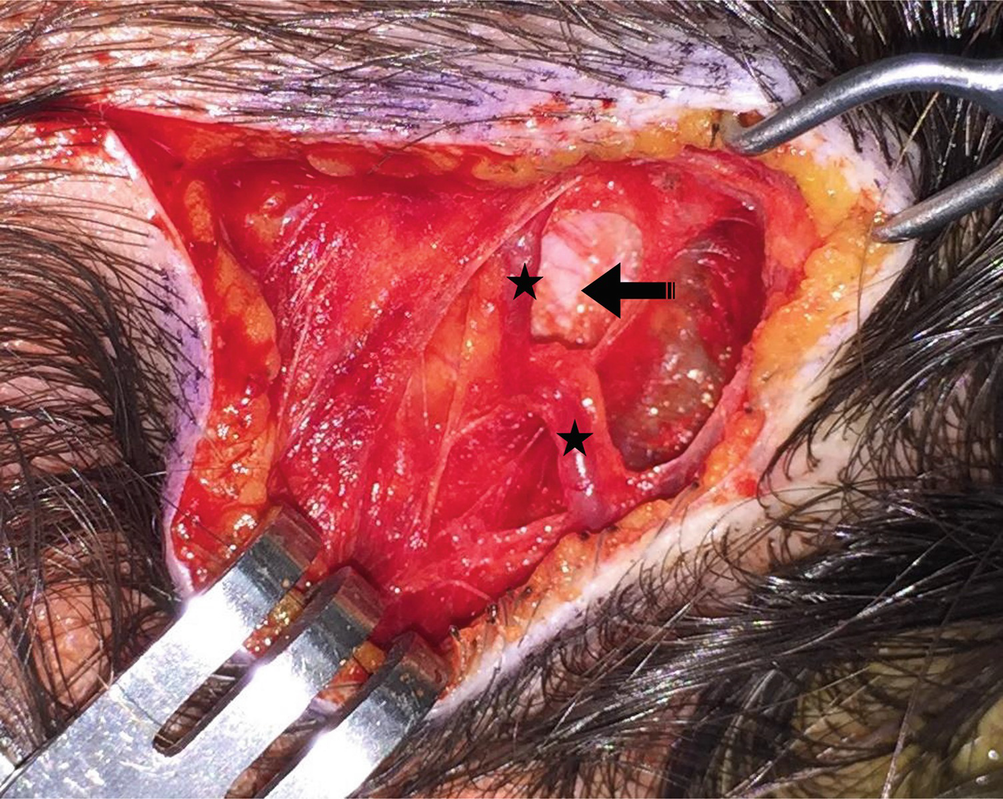
Bifurcated occipital artery (stars) lying above the occipital nerve (arrow)
Aneurysmatic occipital artery (star) running cephalad to the greater occipital nerve (arrow)
Dilated occipital artery (star) running caudal to the greater occipital nerve (arrow)
Related posts:
 Approach for Auriculotemporal Nerve Decompression, Amirlak Modification
Approach for Auriculotemporal Nerve Decompression, Amirlak Modification
 Anatomy of Craniofacial Nerves Regarding Migraine Surgery
Anatomy of Craniofacial Nerves Regarding Migraine Surgery
 Regional, Targeted (ART) Botulinum Toxin Injection for Migraine and Chronic Headaches
Regional, Targeted (ART) Botulinum Toxin Injection for Migraine and Chronic Headaches
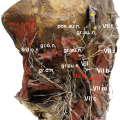 Anatomy of the Vascularization and Innervation of the Human Scalp
Anatomy of the Vascularization and Innervation of the Human Scalp
 of Frontal Trigger Sites
of Frontal Trigger Sites
 of Temporal Trigger Sites
of Temporal Trigger Sites
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


