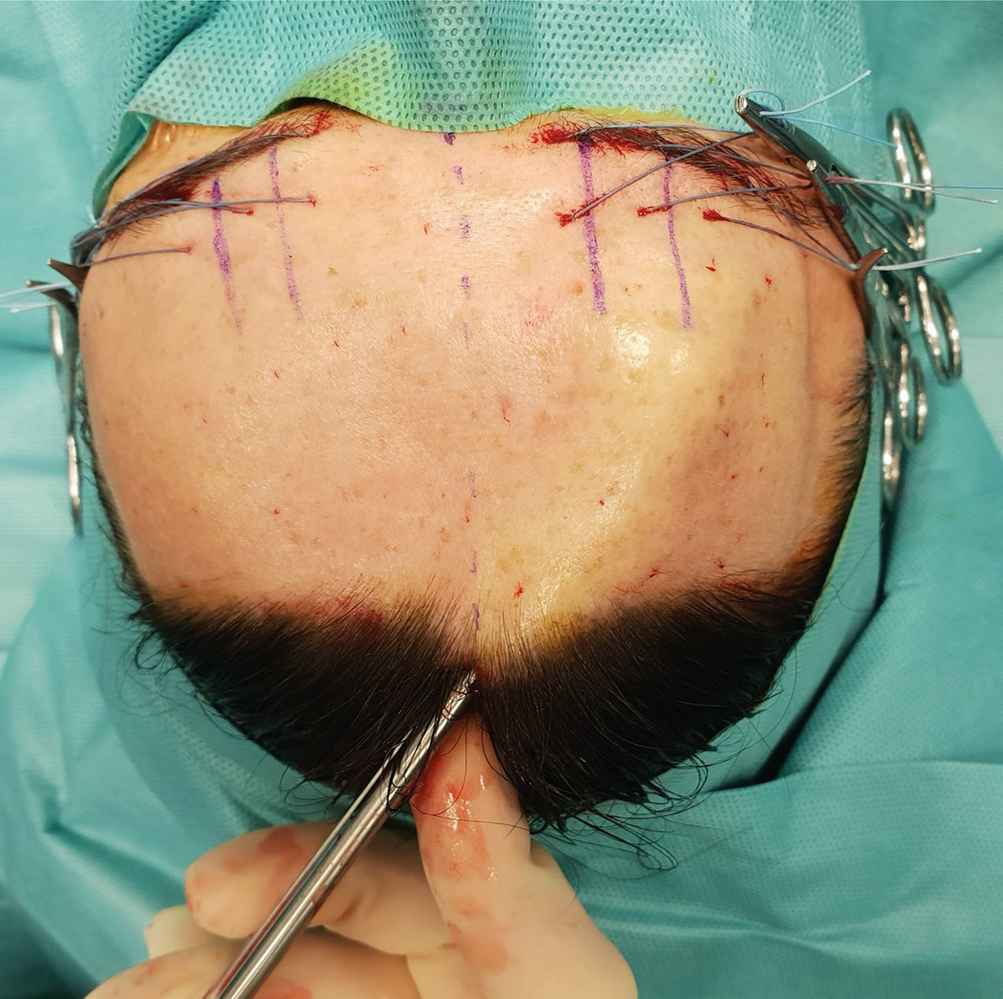
Preoperative markings showing the position of the supraorbital nerve (SON) at the mid-pupillary line and the supratrochlear nerve (STN) at 1.5–1.7 cm from the midsagittal line. This is very helpful to orient the endoscope tip during the procedure and to avoid nerve injuries

Surgical devices for endoscopic myotomies. For this minimally invasive, single-entry technique, it is necessary to use a modified endoscope with fibre light transmission and a wire loop for electrocautery at the distal end

We recommend performing first peripheral nerve block by injecting small amount of anaesthetic solution at the exit of SON and STN at about 5–6 mm above the medial aspect of the eyebrow

Infiltration with diluted anaesthetic solution (40-cc Carbocaine 1% + 40-cc NaCl 0.9% and 20-cc sodium bicarbonate) facilitates the dissection of the submuscular plane. We recommend placing the needle tip just above the periosteum of the frontal bone

Once the area is infiltrated with local anaesthetic, the eyebrows are pierced with suspension sutures (1-0 nylon or silk) to further elevate the dissection plane during the procedure

The second operator pulls up the suspension sutures. This manoeuvre eases endoscope insertion and visualization of the operatory field. In our experience this technical tip did not cause any nerve injuries and it did not elicit post-operative pain
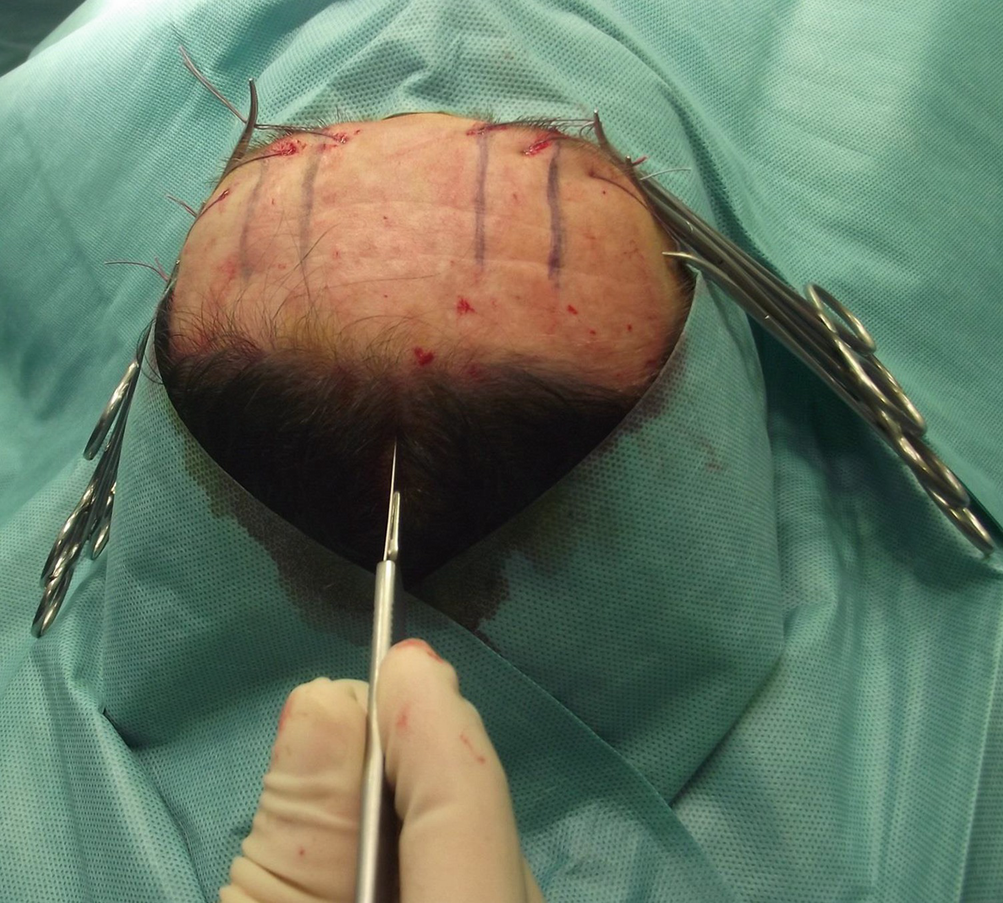
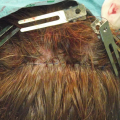
Midline 1.5 cm long incision. Note the location just 1–2 cm behind the hairline in order to mask the resulting scar. The scalpel should be kept parallel to hair bulbs to prevent follicle injuries and avoid the risk of scarring alopecia at the entry site
Sovraperiosteal undermining

Endoscope insertion through the skin incision. Note the function of suspension sutures on the eyebrows

Operative setting
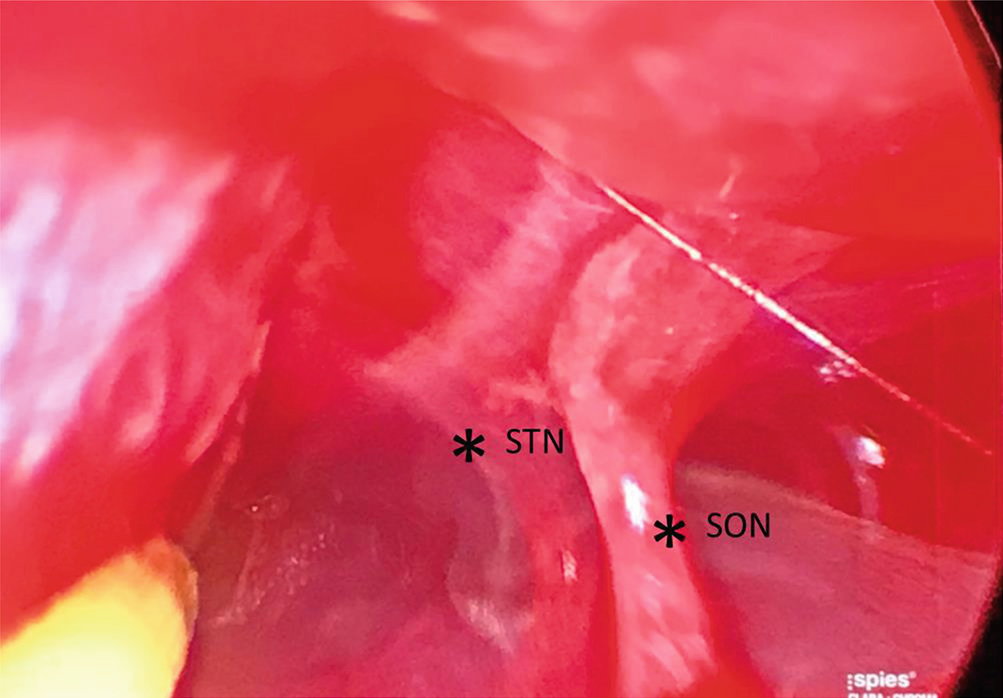
Endoscopic visualization of the supratrochlear nerve (STN, on the left) and the supraorbital nerve (SON, on the right)

Wire loop for electrocautery installed on the tip of the endoscope performing myotomies of the right corrugator supercilii, laterally to the supraorbital nerve
Related posts:
 Approach for Auriculotemporal Nerve Decompression, Amirlak Modification
Approach for Auriculotemporal Nerve Decompression, Amirlak Modification
 Anatomy of Craniofacial Nerves Regarding Migraine Surgery
Anatomy of Craniofacial Nerves Regarding Migraine Surgery
 Regional, Targeted (ART) Botulinum Toxin Injection for Migraine and Chronic Headaches
Regional, Targeted (ART) Botulinum Toxin Injection for Migraine and Chronic Headaches
 Anatomy of the Vascularization and Innervation of the Human Scalp
Anatomy of the Vascularization and Innervation of the Human Scalp
 of Temporal Trigger Sites
of Temporal Trigger Sites
 of Occipital Trigger Sites
of Occipital Trigger Sites
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


