Optimization of resistance to infection, growth, sexual maturation, wound healing, and provision of the best possible overall quality of life are important management goals in children with epidermolysis bullosa. However, all these goals rely on the maintenance of optimal nutritional status, and achieving this is extremely challenging in the severe types of the disease. Strategies to improve nutritional status have the best chance of success when the dietitian or nutritionist works as an integral member of the multidisciplinary team and is well informed of patients’ situations, family dynamics, and prognoses. Even the best-coordinated dietetic interventions may exert only limited impact.
Optimization of resistance to infection, growth, sexual maturation, wound healing, and provision of the best possible overall quality of life are important management goals in children with epidermolysis bullosa (EB). However, all these goals rely on the maintenance of optimal nutritional status; and achieving this is extremely challenging in the severe types of EB. Unless a multiplicity of factors, such as inadequate skin care, poor dentition, esophageal stricture, gastroesophageal reflux (GER), painful defecation, and psychological and psychosocial issues are addressed by the collective expertise of the specialist multidisciplinary EB team (MDT), nutritional interventions are destined to founder.
The dearth of published data regarding nutritional support and nutritional requirements in children with EB means that current practice relies on extrapolation from other conditions and expert clinical experience. Strategies to improve nutritional status have the best chance of success when the dietitian or nutritionist works as an integral member of the MDT and is well informed of patients’ situations, family dynamics, and prognoses. However, in the more severe forms of EB, the burden of caring for children with such a distressing and life-limiting condition can be immense; and parents have to prioritize numerous aspects of care. Even the best-coordinated dietetic interventions may exert only limited impact.
Nutritional compromise
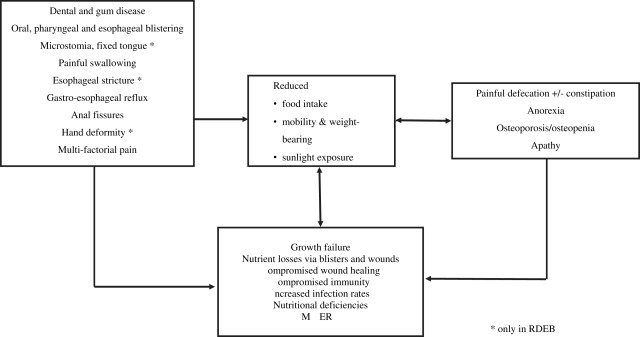
Nutritional compromise corresponds to EB severity, and occurs mainly in generalized forms of recessive dystrophic EB (RDEB) and junctional EB (JEB). In these patients, multiple organ system involvement affects the child physically and psychologically, directly and indirectly. Fig. 1 illustrates the interactions between causes and effects of inadequate nutritional intake in severe EB. In the Dowling-Meara subtype of EB simplex, infants and younger children often experience difficulties in maintaining satisfactory nutritional status and growth. However, in these EB types, excess weight is commonly gained in the preteenage and teenage years because lesions become mainly confined to feet and enforce a predominantly sedentary lifestyle, whereas factors that had previously caused poor oral intake diminish.
Nutritional compromise is a consequence of
- •
The hypercatabolic inflammatory state, in which open skin lesions with consequent losses of blood and serous fluid, increased protein turnover, heat loss, and infection all contribute to increased requirements. As in the patient with thermal burns, nutrient needs reflect the severity of lesions
- •
The degree to which oral, oropharyngeal, esophageal, and other gastrointestinal (GI) complications limit intake or affect absorption. Fecal loading and painful defecation (with or without chronic constipation) are extremely common and frequently cause apathy and secondary anorexia.
Related posts:
 How to Take Skin Biopsies for Epidermolysis Bullosa
How to Take Skin Biopsies for Epidermolysis Bullosa
 Epidermolysis Bullosa Simplex with Muscular Dystrophy
Epidermolysis Bullosa Simplex with Muscular Dystrophy
 Genitourinary Tract Involvement in Epidermolysis Bullosa
Growth and Pubertal Delay in Patients with Epidermolysis Bullosa
Genitourinary Tract Involvement in Epidermolysis Bullosa
Growth and Pubertal Delay in Patients with Epidermolysis Bullosa
 Epidermolysis Bullosa Care in Germany
Epidermolysis Bullosa Care in Israel
Epidermolysis Bullosa Care in Germany
Epidermolysis Bullosa Care in Israel
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


