Nose (Cancer and Reconstruction)

Description
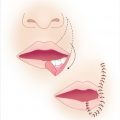
Full-thickness defect of the sebaceous skin covering the nasal tip.
The structural framework and nasal lining are not violated.
The defect measures < 1.5 cm in size, which is appropriate for local tissue transposition.
Involves one nasal subunit, the tip, but does not violate the remaining aesthetic subunits.
Work-up
History
History of sun exposure.
Personal or family history of skin cancer.
Inherited predisposing conditions
Xeroderma pigmentosum, Muir-Torre syndrome, Gorlin syndrome, albinism, basal cell nevus syndrome, others.
Diagnostic studies
Full-body integument examination.
If patient presents initially without previous treatment, a biopsy should be performed at the time of evaluation to establish a diagnosis.
Full-thickness incisional versus excisional biopsies may be performed. Avoid shave biopsies.
Treatment
Consider Mohs surgery consultation, if available.
Allows examination of ~ 100% of surgical margins; highest cure rates.
Board examiner may require that you excise this yourself.
Excision (see Table 6.1)
Basal cell carcinoma: 2- to 5-mm margin. Larger margin for aggressive subtypes.
Squamous cell carcinoma
4 mm if lesion < 2 cm, well-differentiated, not invasive.
6 mm if lesion > 2 cm, poorly differentiated, invasive into fat, or in high-risk location (central face, ears, scalp, hands, feet, genitalia).
Melanoma: Excision margins determined by Breslow thickness.
In situ: 5-mm margin.
< 1 mm: 1-cm margin.
1 to 2 mm: 1- to 2-cm margin.
> 2 mm: 2 cm margin.
Stage II melanoma (depth > 2 mm or > 1 mm with ulceration) may require sentinel lymph node biopsy (surgical oncology consultation).
Stage III melanoma (positive lymph nodes) may require interferon (medical oncology consultation).
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


