Nonsurgical Tightening Procedures
Sorin Eremia
Important Differences between Lighter and Darker Skin Types
The detailed histologic and physiologic characteristics of darker skin types are beyond the scope of this chapter.1,2,3, and 4 Chapter 2 provides an overview of the structural and physiologic features of darker skin types. It is, however, important to understand three key differences between lighter and darker skin types that are relevant to the aging process and to methods of skin tightening discussed in this chapter.
Presence of increasing amounts of melanin
The amount of melanin is the very basis of the skin type I to VI classification. More melanin translates, on one hand, into better photoprotection and delays the appearance of the photoaging changes seen earlier in lighter-skinned individuals. On the other hand, melanocyte response to epidermal and superficial dermal tissue injuries is more severe, with potential permanent or at least long-lasting and difficult-to-treat pigmentary changes. Therefore, when aging changes begin to appear in darker-skinned individuals and these patients seek treatment, much greater care must be taken when using the concept of tissue injury to trigger rejuvenating changes, such as new collagen and elastic tissue formation and collagen tightening and remodeling in general.
Treatment methods that involve significant epidermal tissue injury, methods that are defined as ablative skin resurfacing—be they the more modern laser or broadband light-based methods or the older chemical and mechanical abrasive methods—are not well suited for darker skin types. Such treatment techniques are in fact considered largely contraindicated for anyone with skin darker than what is defined as a relatively light type IV. The increased presence of skin pigment also generally limits the wavelengths that can be used for photorejuvenation treatments to longer wavelengths outside the melanin absorption spectrum. Epidermal cooling to protect superficial skin injury that may trigger melanocytes to respond also becomes of greater importance the darker the skin type that is being targeted for treatment.
Increased thickness of skin associated with dark skin types
The increased thickness of skin associated with darker skin types appears to be primarily due to increased dermal thickness and amounts of collagen present. Combined with better melanin photoprotection, it delays the appearance of fine wrinkles associated with actinic damage, typically seen in lighter skin type individuals. It contributes to differences in skin appearance at a given age, according to skin type characteristics, and makes larger wrinkles a greater concern for non-Caucasian patients, especially those with types V and VI skin. In the author’s experience, thicker, non-Caucasian type skin tends to experience better tightening following the use of nonablative rejuvenating devices that heat the dermis.
Risk of hypertrophic and keloid scar formation and generally greater visibility of incisional scars
These risks make incisional-based, especially traditional long incision, tissue-resection–based skin tightening less desirable for non-Caucasian skin patients. It raises some concerns even for minimal incision lifts, although in the author’s experience, relatively small incisions placed inside the hairline and closed without tension do not present a significant problem. Increased tendency to scar formation also increases the risk of serious complications secondary to heat-generating energy–based nonablative rejuvenating devices, from what would have been only a minor superficial burn in lighter skin type patients. Therefore, greater caution must be exercised with such devices for darker, non-Caucasian patients. Many of the published and conference presented reports of good skin tightening results achieved with such devices also include, in the complications section, a certain number of minor burns that healed without or with minimal scarring. Unless otherwise specifically mentioned in the reports, most likely those injured were lighter skin type patients, and far more serious consequences could have developed in comparably burned darker skin type patients.
As of August 2006, there are two categories of relatively nonsurgical, minimally invasive treatment methods and devices that are available for skin tightening in darker-skinned, non-Caucasian patients: (a) the use of energy-delivering devices to achieve tissue tightening, and (b) the use of minimal incision suspension sutures, including the newer small barbed or larger multianchor type suture. These sutures elevate the tissues into position and rely either on natural postinsertion skin contraction or on inducement of subcutaneous fibrous tracts or fibrosis in a plane above or below the elevated tissues to hold up the lift long term. To improve long-term results, increased tissue fibrosis and contraction is induced through various methods, including the combined use of energy-delivering devices with suspending sutures.
Energy-Delivering Devices Used for Nonablative or Minimally Ablative Skin Tightening
The concept behind these devices is to deliver sufficient energy to the superficial and middermal tissue without creating any—or at least very little—injury to the epidermis, hence the terms nonablative and minimally ablative. The energy is transformed into heat as it is absorbed by the target tissue. The desired thermal injury occurs in the area of maximum energy absorption. The injury triggers formation of new collagen and elastic tissue; it is hoped, in sufficient amounts, to achieve a clinically significant improvement. Sufficient heating of the collagen fibers can also trigger some dermal “remodeling” through instant shrinkage of these protein fibers. The trick is to limit the thermal injury to the targeted dermal tissues and to avoid significant injury to the epidermis, either from direct epidermal absorption of the energy beam as it traverses the epidermis to reach the dermis or from diffusion of the heat superficially. Selection of suitable energy parameters and delivery methods, such as wavelengths and pulse widths, can minimize or virtually eliminate the absorption of energy by the epidermal tissue and determine the depth of maximal dermal absorption. The use of epidermal cooling technologies can protect the epidermis from injury resulting from a certain degree of unavoidable energy absorption by epidermal tissue and from heat diffusing up from the dermis.5
From a wavelength point of view, properly delivered far infrared and radiofrequency energy can pass through the epidermis with very little absorption by epidermal tissue, including melanocytes. Wavelength selection also takes into consideration its scatter characteristics as it passes through tissue. Some wavelengths in the infrared spectrum, such as 1,319 nm and 1,450 nm, also have more scattering characteristics as they penetrate through the dermis than 1,064 nm, so most if not all the energy is delivered to the desired dermal target area. On the other hand, when the target area is deeper—such as with hair follicles, which are deeper in the subcutaneous fat—a wavelength with low scatter characteristics is better suited. The delivery of energy in pulses can also vary the target tissue. Various components of the skin have different thermal relaxation times. Larger targets, related to the surface-to-volume ratio of the target, dissipate absorbed heat more slowly than smaller targets. Therefore, when energy is delivered more slowly over time (longer pulse width), smaller targets with short thermal relaxation times have the time to dissipate the heat before the next pulse of energy hits the target, and the heat does not accumulate. Larger targets, with longer thermal relaxation times, accumulate heat, eventually reaching the critical temperature that triggers thermal injury. Skin-cooling strategies also need to take into account the source of heat reaching the epidermis. When some of the energy is absorbed by the epidermis as it passes through, precooling as well as contemporaneous cooling of the epidermis is very important to prevent epidermal injury. When the heat is not the result of direct absorption by the epidermis but instead rises up from the dermis, postcooling or continuous cooling may be more effective at preventing epidermal injury. Continuous cooling is obviously effective at protecting the epidermis, but on one hand can carry the risk of excessive cooling and freeze injury to the epidermis and on the other hand can diffuse into the dermis and negate the desired thermal injury there.
Although device manufacturers obviously take all such factors into consideration when building their machines, patent restrictions and technical and cost considerations sometimes limit their ability to provide the most effective energy delivery and cooling system. In the author’s opinion, it is important for physicians using such devices to have a thorough understanding of the science behind them to be better able to judge and choose the most appropriate device for the physician’s patient population needs.
First-generation nonablative devices
The first-generation devices specifically designed for nonablative skin tightening were lasers delivering light energy in the far infrared spectrum. CoolTouch (NewStar Lasers, Rosemont, CA) using a 1,320-nm Nd:YAG–generated wavelength and a fixed 50-millisecond pulse width was introduced in 1997. The availability of cryogen spray pre- and postcooling, the addition of a temperature sensor, and a relatively large 10-mm treatment spot set CoolTouch apart from the SmoothBeam (Candela Lasers, Boston, MA), a smaller, less sophisticated, but less expensive, 1,450-nm diode–generated wavelength laser and the European-developed Aramis Erbium:Glass 1,540-nm laser, which never quite caught on in the United States. As is too often the case with new devices, the laser manufacturers and some physicians promoting these lasers made unrealistic claims that as few as four treatments could produce significant skin tightening and improvement in acne scars and even improve acne. In time, it was determined
that many treatments (for example, in the author’s experience, 10 to 14 monthly treatments with the CoolTouch laser) were needed to achieve modest long-term skin tightening or acne-scarring improvement. Overaggressive treatments also resulted in rare but annoying scarring thermal injuries. Both the CoolTouch and SmoothBeam lasers are still available and have proven to be generally reliable, low-operating-cost lasers. Very similar to the CoolTouch, but technologically more advanced, is a Sciton 1,319-nm Nd:YAG laser that presents several advantages. It has a variable pulse width, which allows great flexibility as to how the energy is delivered; a fast, large treatment area with a scanned 6-mm spot; and excellent adjustable contact window cooling. One of the chief complaints about the CoolTouch, and the SmoothBeam lasers is significant patient discomfort. Use of longer pulse widths decreases treatment pain, and, when compared with the 10-mm CoolTouch spot size, so does the randomly scanned smaller 6-mm Sciton spot. The unit can operate on a platform that can support multiple lasers (such as 1,064-nm Nd:YAG and an Er:YAG, and pulsed broadband light units). The wavelength used by all these lasers has virtually no melanin absorption.
that many treatments (for example, in the author’s experience, 10 to 14 monthly treatments with the CoolTouch laser) were needed to achieve modest long-term skin tightening or acne-scarring improvement. Overaggressive treatments also resulted in rare but annoying scarring thermal injuries. Both the CoolTouch and SmoothBeam lasers are still available and have proven to be generally reliable, low-operating-cost lasers. Very similar to the CoolTouch, but technologically more advanced, is a Sciton 1,319-nm Nd:YAG laser that presents several advantages. It has a variable pulse width, which allows great flexibility as to how the energy is delivered; a fast, large treatment area with a scanned 6-mm spot; and excellent adjustable contact window cooling. One of the chief complaints about the CoolTouch, and the SmoothBeam lasers is significant patient discomfort. Use of longer pulse widths decreases treatment pain, and, when compared with the 10-mm CoolTouch spot size, so does the randomly scanned smaller 6-mm Sciton spot. The unit can operate on a platform that can support multiple lasers (such as 1,064-nm Nd:YAG and an Er:YAG, and pulsed broadband light units). The wavelength used by all these lasers has virtually no melanin absorption.
Other lasers and early broadband light devices
The concept of nonablative thermal skin injury to induce formation of new collagen and elastic tissue led to attempts to use other existing lasers, such as the 595-nm pulse dye laser, the 1,064-nm Nd:YAG with long pulse width, alone or in combination with the 532 Nd:YAG to induce skin tightening. In general, these results have been very modest. The use of the 532-nm and the 595-nm wavelengths in darker skin is contraindicated. The use of selectively filtered pulsed broadband light was also attempted for purposes of skin tightening. The earliest version was the “photofacial” treatment with the Lumenis intense pulsed light units. Skin tightening results were very disappointing. Newer units are discussed below.
Radiofrequency devices
In 1999, the ThermaCool device (Thermage Inc., Hayward, CA) was introduced. Volumetric dermal heating is accomplished using a skin-cooling tip with capacitative coupling monopolar radiofrequency (RF) technology. The device converts electrical energy to RF spectrum wavelength energy. These waves of energy are delivered in monopolar fashion to the skin through a square tip that is also equipped with surface chilling to help cool and protect the epidermis. A coupling gel is used to decrease epidermal impedence and allow the energy to get through to the dermis with minimal absorption. Dermal tissue resistance/impedence converts the RF spectrum energy waves to heat, which has been shown to produce various degrees of tissue-tightening results. FDA approval for periorbital skin tightening use was obtained in 2002 amid much fanfare and claims of impressive documented skin tightening and lateral brow elevation. This was followed with claims on national television shows of impressive tissue tightening and appearance improvement in the jowls area of the face. Unfortunately, these results seemed largely exaggerated, or at best unpredictable, and limited to a small percentage of treated patients. Claims were also made of significant acne scarring improvement as well as long-term improvements in acne as well. Misguided attempts to produce such results through use of high-power settings led to some highly publicized burns with permanent scars.6 The treatment tips initially developed by Thermage were small (1 cm) and delivered the energy slowly and quite painfully. Newer generations of tips and improved treatment protocols that involve multiple passes at lower energy settings7 have decreased risks, improved treatment speed, and, with the most recent 3-mm tips, significantly decreased patient discomfort and operator fatigue. These large tips have also rendered more practical the use of the Thermage unit for nonfacial areas, such as the abdomen and arms, with studies ongoing.
The newest Thermage tip is specially designed for treatment of the eyelids, which was previously contraindicated with the older tips. This tip is much smaller, delivers much less energy, and is designed specifically for the thin upper-lid skin. The use of a plastic (not metal) eye shield is essential. The eyelid tip was introduced in April 2006, and preliminary results appear to be better and more predictable than results on the face. Because RF waves are not absorbed by melanin, non-Caucasian skin is well suited to it (Fig. 21-1A,B). Also, the thicker dermis of certain ethnicities appears to respond better to this device than thinner skin. The cost of the ThermaCool unit is much lower than most other tissue-tightening devices. It is relatively small and portable as well as reliable and less expensive to maintain than laser and light units. However, the cost of the tips, which are single-use disposable devices, is quite high—$500 to $600 or more per treatment (about $175 for the eyelids tip)—and has been one of the obstacles for greater use. Thermage was once promoted its product as an independent, one-time, effective treatment. More likely, several treatments at 1- to 3-month intervals are needed for best results. Although not as much a concern with types V to VI skin, the RF-induced skin-tightening effects do little if anything for fine facial wrinkles nor does it improve any pre-existing dyschromia. The author is using Thermage both as an independent procedure and in combination with the knotted multianchor suspension suture lift (AnchorLift) discussed later in this chapter.
In 2005, Aluma (Luminis, Santa Clara, CA) introduced a bipolar RF unit using vacuum to press the tissues to the treatment head. This keeps the skin in contact with the parallel electrodes, decreasing the risk of arcing and accidental skin burns. It is claimed this vacuum-negative pressure, which pulls the tissues tight onto the RF current–generating electrodes, reduces the fluences needed to heat the desired
volume of dermis, reducing patient discomfort. As with other RF units, a coupling gel is also used.
volume of dermis, reducing patient discomfort. As with other RF units, a coupling gel is also used.
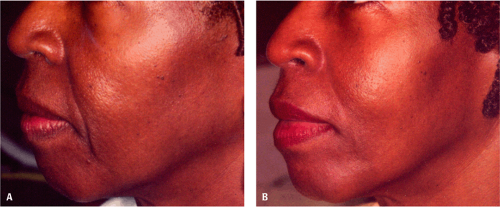 Figure 21-1 A: Pretreatment of lower face rhytides, type VI skin, African American patient. B: Six months posttreatment of the lower face with a Monopolar RF device. (Courtesy of Dr. Mark Nestor and Thermage Inc.) |
The tip is disposable and works for only 300 pulses, rendering treatment costs relatively high. The initial manufacturer-supported studies claim impressive results, but, as with most of these units, early results have yet to be independently confirmed as truly clinically significant.
Accent (Alma Lasers, Caesarea, Israel), still awaiting FDA approval, has two separate handpieces—one for monopolar and one for bipolar RF technology—to provide variable penetration depths and heating. The monopolar handpiece heats the dermis up to 2 mm in depth and appears to be designed for tissue tightening. The bipolar handpieces heats deeper, between 2 and 4 mm, and may be able to cause adipocyte lipolysis. The released fatty components are absorbed and eliminated. The bipolar component is more designed for treatment of cellulite. Treatment pain has been reported to be a significant factor, and results are variable. The unit is thus a dual-purpose one, designed to induce facial skin tightening and for treatment of cellulite on the rest of the body. Care must be taken not to use the bipolar component on the face where it could lead to subcutaneous fat loss. Alma also makes a fractional delivery device (Pixel) using an Er:YAG laser (not to be confused with the Er:Glass lasers used by Fraxel and Palomar) and a pure pulsed broadband light device.
Combined radiofrequency and broadband light devices
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


