Nipple Reconstruction
Kasandra Dassoulas
Brendan Collins
Bernard W. Chang
DEFINITION
Nipple reconstruction is the final stage in breast reconstruction and allows the reconstructed breast to most closely resemble the natural breast.
There are many different techniques used to reconstruct the projecting portion of the nipple-areolar complex; those reviewed in this chapter form the basis for many other techniques.
ANATOMY
The nipple-areolar complex is an average of 4 cm in diameter, the nipple 1.3 cm in diameter, with the projecting portion 9 mm in length.1
The aesthetic ideal for the location of the NAC is at the apex, or most projecting aspect of the breast mound.
PATIENT HISTORY AND PHYSICAL FINDINGS
Nipple reconstruction should be offered to appropriate candidates, generally as the final step in the breast reconstruction process.
Nipple reconstruction is typically performed at least 3 months after either autologous or final implant placement to allow incisions to completely heal and the shape of the reconstruction to stabilize.
Presence and location of previous scars from breast reconstruction should be noted.
The presence of a scar across the breast mound and its location may influence the chosen reconstructive technique and decisions regarding placement.
Thickness of the skin and subcutaneous tissue as well as a history of radiation should be noted.
In the case of implant-based reconstruction, if the soft tissue overlying an implant is excessively thin or damaged from prior irradiation, nipple reconstruction may carry a greater risk for skin necrosis, infection, and implant exposure.
Under these circumstances, surgical nipple reconstruction should not be offered or should be offered with caution. The patient may still be a candidate for tattooing alone.
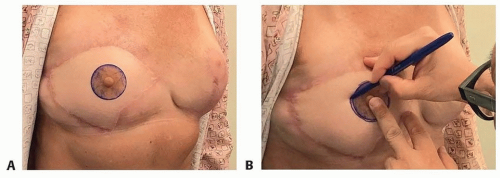 FIG 1 • A. Silicone nipples or telemetry pads can be used to mark the site of the new nipple. B. The silicone nipple can be traced to form the outside of the keyhole pattern. |
NONOPERATIVE MANAGEMENT
Tattooing without reconstruction of the projecting portion of the nipple is a nonsurgical option.
SURGICAL MANAGEMENT
Once the decision has been made to pursue nipple reconstruction, the surgeon must decide whether this will be combined with other revisionary procedures. This may dictate the operative setting and anesthetic requirement, that is, office vs outpatient surgery.
Nipple reconstruction alone can often be accomplished in the office with local anesthesia.
Preoperative Planning
The location of the new nipple to be reconstructed is marked preoperatively with the patient standing, oftentimes in front of a mirror to allow for patient feedback.
Silicone nipples or telemetry pads can help illustrate the reconstructed nipple location (FIG 1A,B).
Positioning
For unilateral reconstruction, the nipple position will reflect the contralateral nipple position. If a contralateral symmetry procedure is needed, which will change the position of the native nipple, that is, reduction or mastopexy, the reconstructed nipple will reflect this new position.
The operation is performed with the patient in a supine position with arms abducted 90 degrees or tucked at the patient’s sides. The patient should be positioned with the option to elevate to a sitting position if desired.
Approach
Chosen technique may be based on nature and location of existing scars, as well as surgeon preference. All techniques are associated with the tendency for soft tissue contraction and decrease in nipple projection.
TECHNIQUES
▪ Star Flap
The star flap produces a moderately projecting nipple and minimal flattening of the breast mound but does not offer projection of an areola or circular border.
Three limbs are designed around a central portion (TECH FIG 1A). The central portion base width determines the width of the nipple. The length of the limbs of the star is based on the size of the contralateral nipple or a width of 4 cm if there is no nipple present. The scars can be included in a tattoo at a later point in time that will help to camouflage them.
The lateral wings of the flap are elevated sharply in a subdermal plane (TECH FIG 1B).
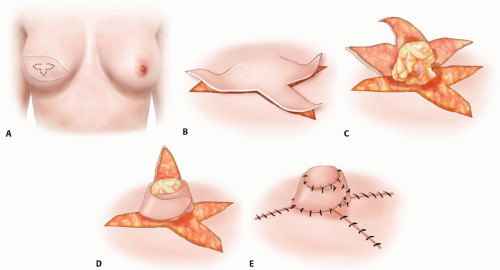
TECH FIG 1 • A. Basic design of the start flap. B. The lateral wings are elevated in a subdermal plane. C. The central wing is elevated subdermally, progressively recruiting subcutaneous tissue to add bulk. D. The lateral wings are wrapped around the central base. E. The central wing is closed over top. The donor sites are closed primarily.
The central wing of the flap is elevated distal to proximal including a gradient of subcutaneous fat with the most at the central base, serving as the bulk of the nipple (TECH FIG 1C).Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree