■ A donor site is chosen for the full-thickness skin graft, which will be used to reconstruct the areola. Commonly used sites include the lateral edge of the mastectomy scar, the lower abdomen, and the groin crease. Additionally, the areolar graft can be taken adjacent to any of the patient’s existing scars.
■ A 38- or 42-mm nipple sizer is used to mark the areolar skin graft. An ellipse is drawn tangent to the areolar graft to allow linear closure of the donor site.
■ The areolar skin graft is scored with a knife prior to harvest. The ellipse is then excised as a full-thickness skin graft (FIG 2).

■ The areolar graft is aggressively defatted with a small sharp scissor, leaving only full-thickness skin behind (FIG 3).

■ The skate flap is designed at the previously marked site (FIG 4).
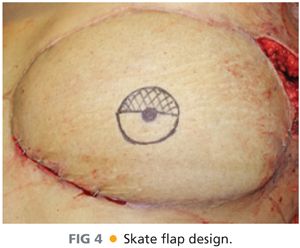
■ A 1- to 1.5-cm circle is drawn at the planned location of the nipple.
■ A 38- or 42-mm nipple sizer is used to mark the areola centered around the nipple.
■ A horizontal line is drawn across the circle at the superior edge of the marked nipple.
■ The upper portion of the circle is crosshatched to mark the area that will be de-epithelialized.
■ The lower portion of the circle will be raised as the “skate flap” to create the new nipple.
■ The epidermis is scored along all incisions.
■ The crosshatched semicircle is de-epithelialized (FIG 5).

■ The flap is then raised from the edges at the level of the middermis. The deepest layer of dermis is left down in order to provide a vascularized bed for the areolar skin graft (FIG 6).

■ The flap remains attached to the deep dermis at the marked nipple. The flap is raised in a slightly deeper plane at the center in order to include some fat with the flap to provide bulk (FIG 7).

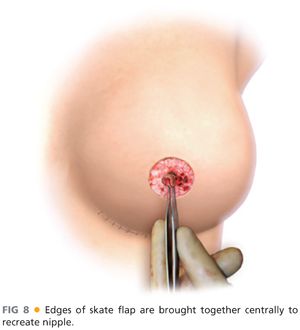
■ The corners of the flap are centralized and sutured to the underlying dermis using 5-0 Vicryl Rapide (FIG 8).
■ The edges of the flap are sutured together using interrupted 5-0 Rapide (FIG 9).

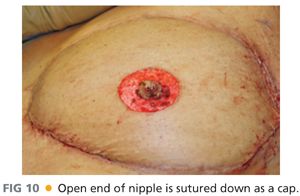
■ The cap is sutured down to close off the nipple (FIG 10).
■ The full-thickness skin areolar skin graft is sutured to the bed using 4-0 chromic half-buried horizontal mattress sutures. The buried portion of suture is placed along the native breast skin to avoid scarring on the breast (FIG 11).

■ A 1-cm hole is cut in the center of the areolar graft to expose the nipple (FIG 12).
Related posts:
 Thyroidectomy for Substernal Goiters
Thyroidectomy for Substernal Goiters
 Inguinal Lymph Node Dissection (Inguinofemoral and Ilioinguinal) for Metastatic Melanoma
Inguinal Lymph Node Dissection (Inguinofemoral and Ilioinguinal) for Metastatic Melanoma
 Thyroid Lobectomy
Thyroid Lobectomy
 Pedicled Transverse Rectus Abdominis Myocutaneous Flap Breast Reconstruction
Pedicled Transverse Rectus Abdominis Myocutaneous Flap Breast Reconstruction
 Free Transverse Rectus Abdominis Musculocutaneous Flap Reconstruction after Mastectomy
Free Transverse Rectus Abdominis Musculocutaneous Flap Reconstruction after Mastectomy
 Subtotal Parathyroidectomy or Total with Autologous Graft
Subtotal Parathyroidectomy or Total with Autologous Graft
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


