Figures for botulinum neurotoxin A procedures in the USA over the past 21 years according to the American Society of Plastic Surgeons [6]
For some slightly inexplicable reason, perhaps due to its rapid growth, BoNT has acquired a certain negativity of reputation in the media that appears undeserved given its extremely good safety profile. Moreover, the majority of contemporaneous research is now directed at the validation of BoNT as therapeutic agents, rather than simple wrinkle erasers, and such uses first outweighed cosmetic, accounting for about 60% of worldwide sales, in 2004. Being such a fascinating entity, BoNT research efforts have yielded a wealth of positive spin-offs, including elucidation of neuronal transport, protein-protein interactions and transmembrane transport systems.
7.2 Basic Facts
Botulinum neurotoxin is the most acutely lethal toxin known, with an estimated human median lethal dose (LD50) of 1.3–2.1 ng/kg intravenously or intramuscularly and 10–13 ng/kg when inhaled [1].
Some characteristics of known botulinum neurotoxin subtypes and their molecular targets
Serotype | Potency | Duration | Common brands | Identified in | SHARE target |
|---|---|---|---|---|---|
A | Highest | Longest, 4–6 months | Dysport®, Botox®, Xeomin® | Human | SNAP-25 |
B | 1/200th A | 6 weeks | NeuroBloc or Myobloc | Human | VAMP1,2 cellubrevin |
C 1 | 1/10th A | Chicken | Syntaxins 1–3, SNAP-25 | ||
C 2 | 1/10th A | Chicken | Syntaxins 1–3, SNAP-25 | ||
D | Cattle | VAMP1,2 cellubrevin | |||
E | Human | SNAP-25 | |||
F | 4–5 weeks | Human | VAMP1,2 cellubrevin | ||
G | Soil | VAMP1,2 cellubrevin |
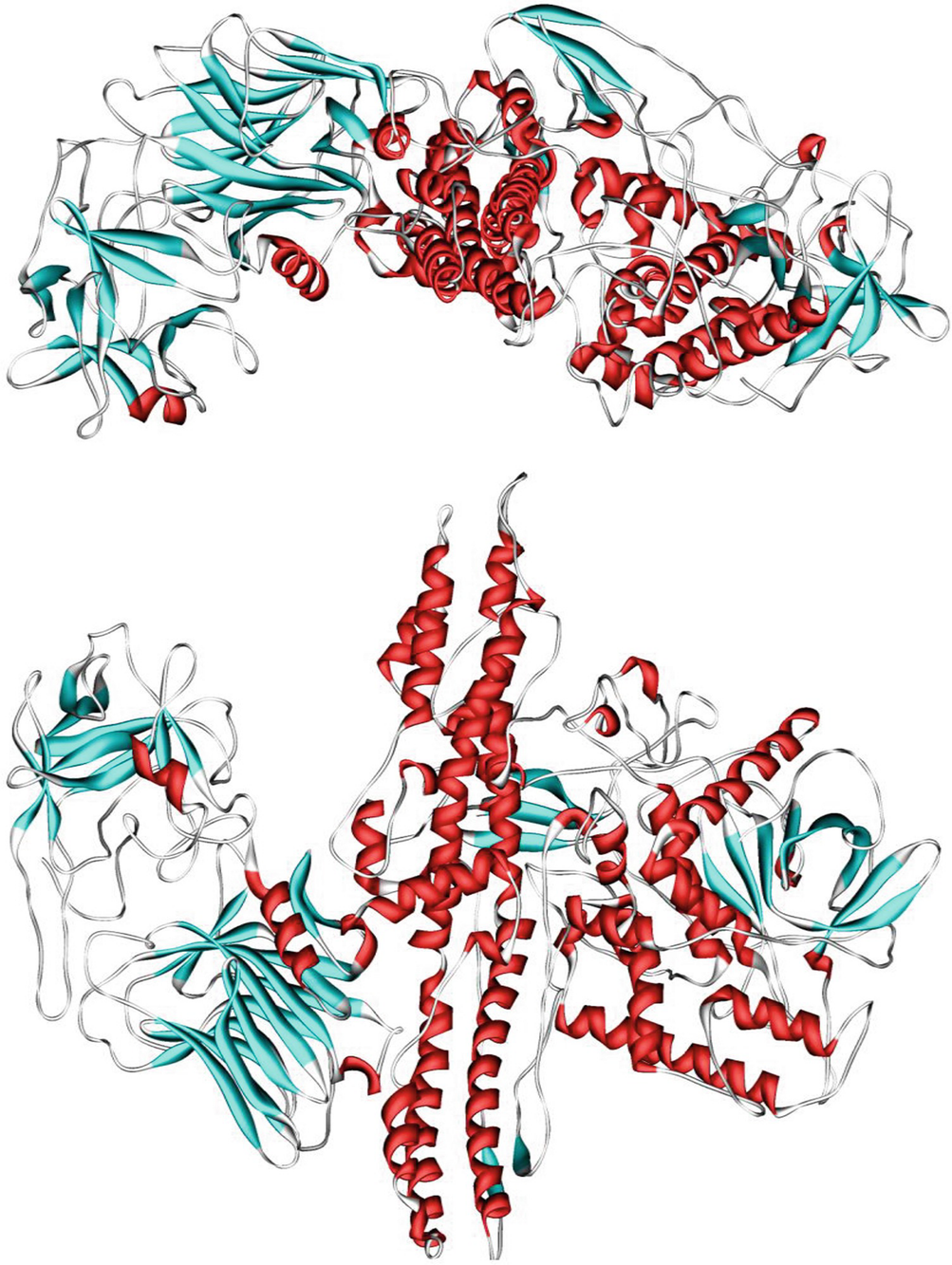
Ribbon structure of botulinum neurotoxin A, generously released into the public domain by the authors [10]
The most common clinical manifestation is food-borne botulism, a severe food poisoning resulting from the ingestion of neurotoxin-containing foods, usually subtypes A, B and E. Whilst spores are heat-resistant, permitting survival in inadequately processed foods, the toxin itself is heat-labile and easily denatured by boiling [14]. Clinical symptoms typically present 18–36 h after ingestion and include marked lassitude, weakness and vertigo, usually followed by double vision and progressive difficulty in speaking and swallowing. Difficulty in breathing, weakness of other muscles, abdominal distension and constipation are also common. A far less well-known and fortunately rare variant, infant botulism, usually occurs from soil particles or honey. It was first described nearly 50 years ago [15] and over 4000 cases are known. Symptoms include the inability to suckle, constipation and general floppiness. Management comprises supportive measures and antitoxin administration.
With approximately 700 reported global cases, the third entity, wound botulism, includes a similar symptomatology to food-borne, but without any gastrointestinal features. Formerly predominantly traumatic in aetiology, it now most often appears in IV drug abusers and has an incubation period somewhat longer at 7–14 days. Cases tend to involve subtypes BoNT-A and BoNT-B.
It is important, however, to appreciate that BoNT-A has different consequences when injected superficially and the standard vial of BoNT-A has 2 × 10−8 or 200 million times, less than the lethal dose [16].
7.3 Physiology and Pharmacology
Neuromuscular blockade was first elucidated as the mechanism of action in 1949 [17]. The resulting flaccid paralysis occurs via a complex, transmembrane inhibition of neurotransmitter (NT) release at peripheral cholinergic neuromuscular junctions. The carboxyl terminal of the ‘heavy’ chain must first bind to unmyelinated, presynaptic cholinergic neurons [18]. Rather quaintly, it has been described as a ‘chaperone’, perhaps forming a protein channel that facilitates membrane translocation of the light chain [19]. With its zinc-dependent proteolytic activity, the 50 kDa moiety specifically degrades cytosolic SNAP (synaptosomal-associated protein)-25. SNAP receptors are found on both vesicle and plasma membranes and are essential for acetylcholine release from the presynaptic terminal of the neuromuscular junction (NMJ) [20].
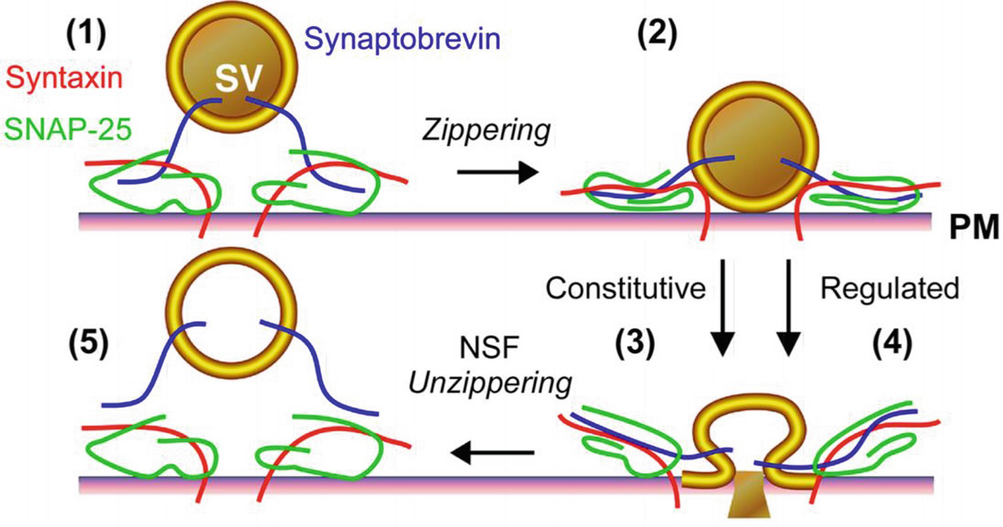
‘Zippering’ as a mechanism for exocytosis as imagined by Lagow et al. and used under the aegis of Open Access [21]
BoNT possesses a number of favourable pharmacological properties, including high potency—allowing small doses to be effective—and a limited local diffusion that depends upon volume [24]. High affinity is evidenced by minimal circulating toxin (10−12–10−14 M) during active botulism. Finally, whilst highly neuro-specific an interesting human volunteer study showed it not to be neurotoxic [25]! Even more interesting is reversibility with time. Although the chemical effect is permanent, axonal regeneration restores clinical function. Unlike most toxins, BoNTs are rare in not causing cell death [26] and extensive, long-term clinical experience has failed to demonstrate neurodegenerative sequelae [27].
As often occurs, the first product eponymises the market and Allergan’s BoNT-A, Botox® (Allergan, Marlow International, Bucks., UK: data insert [28]) removed a useful elision in the form of Botulinum Toxin from common parlance. Whilst the USA favours Botox®, Europeans have used Dysport (Ipsen Biopharm Ltd., Wrexham, UK: data insert [29]) for almost as long. Botulinum toxicity is expressed in units, e.g. BU (Botox® units) or DU (Dysport® units), and one unit equates to one LD50 by murine bioassay. A recent entrant—Xeomin (Merz Pharmaceuticals GmbH, Frankfurt, Germany: data insert [30])—comes without the complexing proteins of the other two, and there are a wealth of products originating in China and South Korea. Much research in the 2000s compared Botox® with Dysport® and each side had its proponents. No clear winner emerged and, with differing proprietary formulations, the literature suggested a conversion factor of 2.5–4 × units of Dysport® compared to Botox® [31, 32]. It is now generally accepted that protein complex dissociation is virtually instantaneous at physiological pH so reduced protein load provides a theoretical advantage. All three companies provide their BoNT-A in two volumes, the smaller being intended for single patient use.
7.4 Clinical
With BoNT-A being relatively novel in its application to migraine, its application to cutaneous wrinkle reduction has been far more extensively studied and a few of the fundamentals are worth summarising. Within 30 min of injection, the neurotoxin has diffused through the muscle and the heavy chain has become bound to the axon terminal. Following internalisation of the light chain, zinc-dependent metalloprotease-mediated degradation of cytosolic SNAP occurs to interrupt acetylcholine release from the presynaptic terminal [20]. Clinical effects therefore do not start appearing for 2–3 days. The paralytic effect of BoNT-A is known to be dose related with the peak effect being reached between 5 and 8 days [33].
Histopathological confirmation of atrophy with mild demyelination at the neuron terminal confirms the permanent nature of chemical denervation [34]. Explanation for the clinical effect wearing off after 3–6 months is provided by both synaptic switching [35] and neurogenic axonal sprouting [36]. Perhaps irksome to the uninitiated patient due to the need for repeat administration, reversibility is one of the most important facets of BoNT-A treatment. It is well to remember that any adverse effects will also wear off in time.
Covered elsewhere in greater depth, migraine continues along the serendipitous path of BoNT’s story with FDA approval in October 2010. Original credit goes to Guyuron, a plastic surgeon, who observed a link between BoNT-A administration and migraine alleviation in the mid-1990s [37]. It is not yet fully understood how botulinum toxin works in migraine, but a recent animal study suggested that botulinum toxin inhibits pain through nerve cells in the trigeminovascular system [38].
7.5 Safety and Complications
For a 70 kg adult, the LD50 (the quantity of a chemical fatal in 50% of test subjects) is estimated from primate studies at 40 μm/kg or 2800 U [39]. Given that 50–100 U and 300–600 U are used for cosmetic and medical indications, respectively, safety margins are comfortably wide. Adverse effects of BoNT-A are largely predictable and stem from either an unintended effect of the neurotoxin itself or an allergic reaction to the protein structure. Being rare the latter has been downgraded so egg allergy is now not an absolute contraindication. By 1989 Scott concluded complications to be ‘rare, mild and treatable’ in the main [40]. Alastair Carruthers, one of the original gurus, felt there were really only two significant complications of correct neurotoxin administration: headaches and eyelid ptosis [41]. The former tend to diminish with regular administration and the latter reduce in incidence with injector experience. In a meta-analysis performed in 2004, mild-to-moderate complications occurred in 25%. Whilst this may sound high, placebo treatment caused 15% and both active and placebo produced focal weaknesses that fully recovered [27].
7.5.1 Adverse Effects: Systemic
Related posts:
 Approach for Auriculotemporal Nerve Decompression, Amirlak Modification
Approach for Auriculotemporal Nerve Decompression, Amirlak Modification
 Anatomy of Craniofacial Nerves Regarding Migraine Surgery
Anatomy of Craniofacial Nerves Regarding Migraine Surgery
 Anatomy of the Vascularization and Innervation of the Human Scalp
Anatomy of the Vascularization and Innervation of the Human Scalp
 Modification of Site 4 Decompression: Endoscopic Assisted Decompression of the Greater Occipital Nerve (GON) with Radical Excision of the Occipital Artery
Modification of Site 4 Decompression: Endoscopic Assisted Decompression of the Greater Occipital Nerve (GON) with Radical Excision of the Occipital Artery
 of Temporal Trigger Sites
of Temporal Trigger Sites
 of Occipital Trigger Sites
of Occipital Trigger Sites
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


