The midline and hairline are marked with the patient in sitting position (blue dots). GON and tail of GON is marked based on the patient’s areas of maximal tenderness (shown in Fig. 18.4). The point of maximal tenderness for the GON is located within the hair-bearing scalp. Generally, this point for the LON is behind the posterior border of sternocleidomastoid muscle (green dots)

The patient is intubated and then flipped in prone position. All areas of the bed must be padded, with a papoose sheet underneath the Wilson frame and a pillow with mirror (ProneView Prone Head Positioning System with Low Profile Mirror Platform) which facilities visualization of the endotracheal tube and correct positioning of the face

The shoulders are taped back under tension to provide better access to the GON and LON incisions, which is extremely important in high-BMI patients
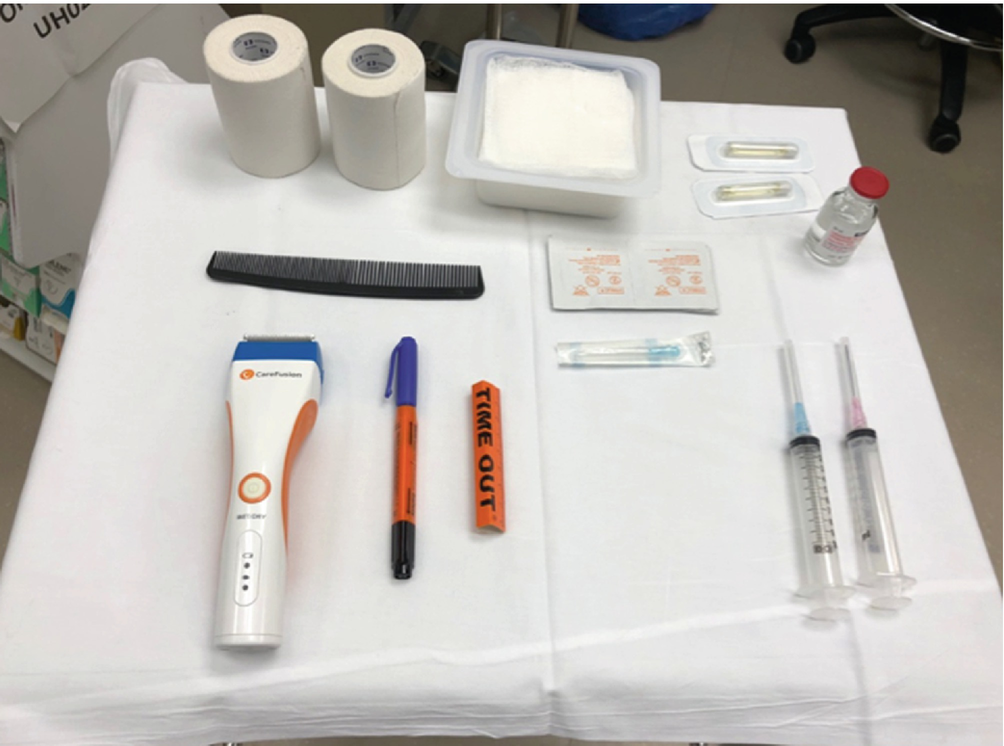
A table that includes equipment for shaving, comb, cloth tape, and injection of epinephrine solution is prepared prior to skin prep

Other instruments required include (from top left): Adson-Beckman retractors, Weitlaner retractor, Obwegeser retractors of varying size, protected bipolar cautery, 30-degree endoscope, skin hooks, scalpel, forceps, fine tonsils, and right-angle forceps
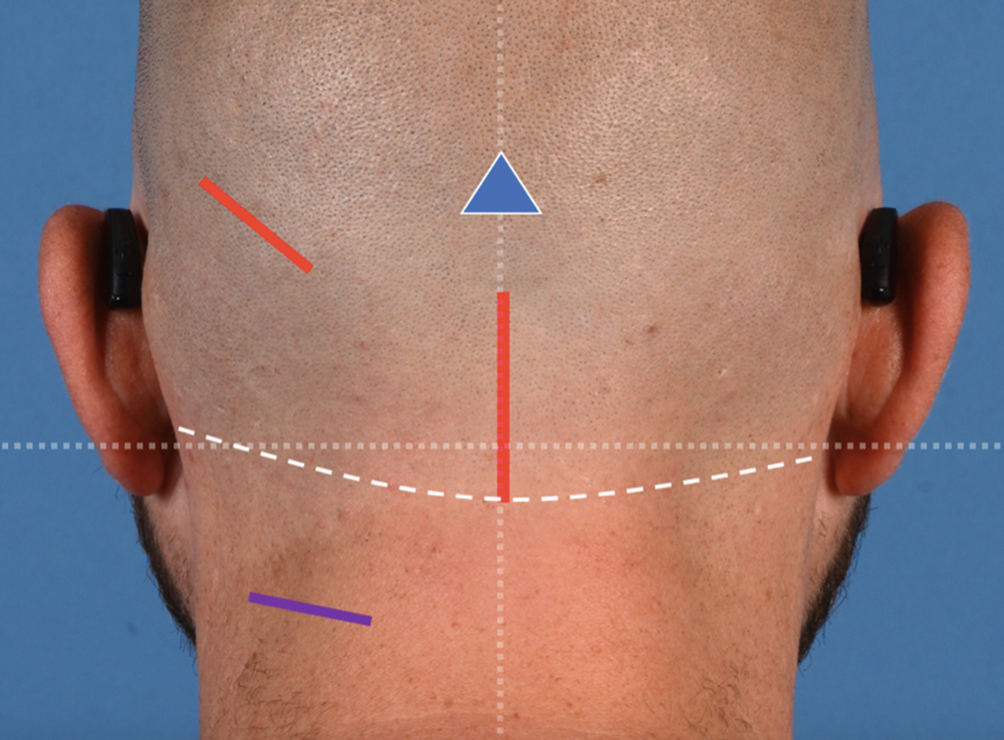
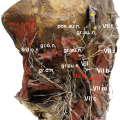
Schematic figure of the GON and LON incisions: midline incision for GON decompression, and the counter-incision to assist endoscopic visualization and excision of distal end of the GON artery is indicated in red. The mid-lateral incision for LON decompression is represented by the purple line

This image shows approximate key locations: midline incision (solid blue), occipital artery (red), LON and GON (green) showing their proximal emergence points and their tail area, all four marked by a green dot based on palpation of the tender anatomical points

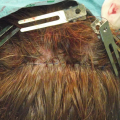
A 3–4 cm incision is made beneath the occipital protuberance within the hairline. Dissection is carried down to the trapezius fascia

The third occipital nerve (held by forceps) when encountered here and can be safely avulsed using hemostat-assisted traction neurectomy. It is important not to confuse a large third occipital nerve with the GON by paying attention to its depth in relation to the trapezius fascia and semispinalis muscle
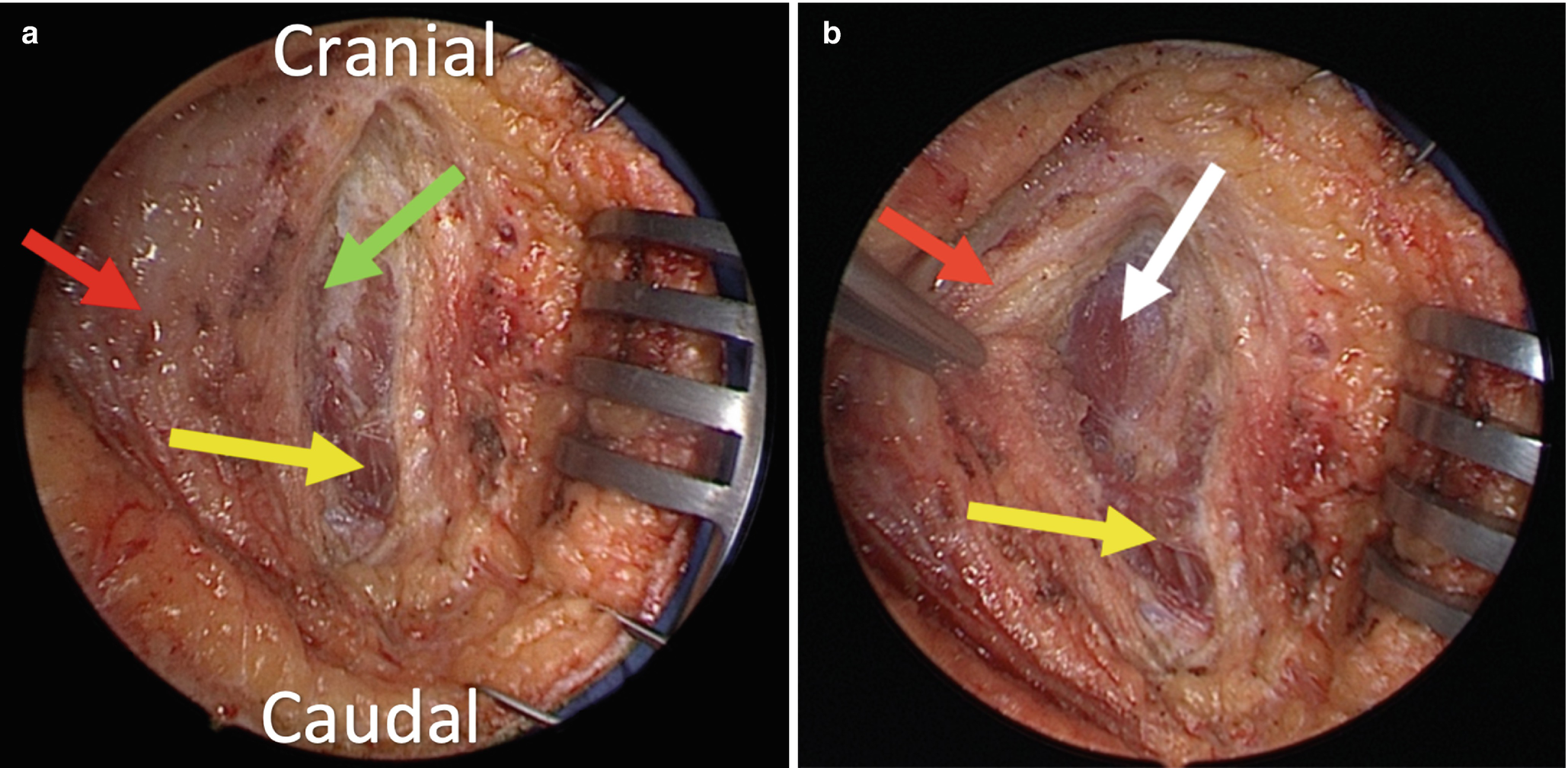
(a, b) The trapezius and semispinalis capitis muscles must be differentiated (this image represents the right side of the neck). This will help to orient the surgeon and facilitate identification of the GON nerve. Commonly, there is midline extension of the trapezius muscle to the midline. Lateral to the midline raphe, the oblique fibers of the trapezius muscle (yellow arrow in both images) are first encountered with another fascial layer under it and over the semispinalis capitis muscles after the going through with trapezius muscle with electrocautery (white arrow in second image) (red arrow = trapezius fascia of midline raphe). The semispinalis muscle, which is deep to the trapezius muscle and fascia and can be identified by its vertical fibers, lighter color, and bulkier appearance when compared to trapezius
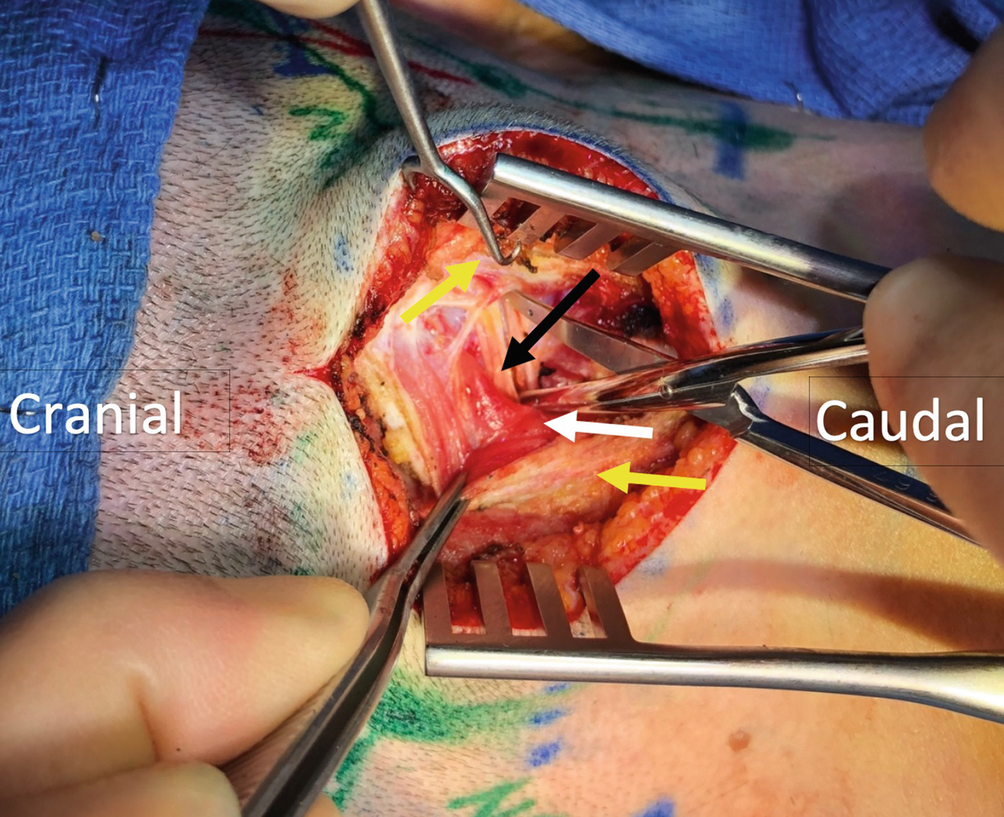
After identification of the semispinalis capitis muscles, blunt dissection is done toward the skin marking in the plane between the trapezius and semispinalis muscles. There should be no digging in the semispinalis capitis muscles to look for the proximal part of the nerve. The trunk of the GON (black arrow) emerges approximately 1.5 cm lateral from midline and 3 cm inferior to the occipital protuberance, but the lateral point of emergence can vary, and one should rely on tactile palpation of the lateral tender area rather than the anatomical location (white arrow, semispinalis muscle fibers; yellow arrow, trapezius fascia)
Related posts:
 Approach for Auriculotemporal Nerve Decompression, Amirlak Modification
Approach for Auriculotemporal Nerve Decompression, Amirlak Modification
 Anatomy of Craniofacial Nerves Regarding Migraine Surgery
Anatomy of Craniofacial Nerves Regarding Migraine Surgery
 Regional, Targeted (ART) Botulinum Toxin Injection for Migraine and Chronic Headaches
Regional, Targeted (ART) Botulinum Toxin Injection for Migraine and Chronic Headaches
 Anatomy of the Vascularization and Innervation of the Human Scalp
Anatomy of the Vascularization and Innervation of the Human Scalp
 of Temporal Trigger Sites
of Temporal Trigger Sites
 of Occipital Trigger Sites
of Occipital Trigger Sites
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


