5
Neuromodulation and Management of Facial Rhytidosis
The concept of relaxing facial muscles and diminishing their secondary wrinkle-producing effects has become a basic technique in facial rejuvenation. It is a foundation on which other noninvasive and surgical procedures can be built (see also Chapters 1, 4, 6, 9, 14, 15, and 16). In selected cases it can be used alone. In others it is an element in the menu of combined therapies. These techniques continue to evolve as new technologies are introduced and our experience with neuromodulating injectables increases.1–9
We instruct our patients and the physicians that we train that the endpoint of treatment is not complete immobilization of the treated muscle. Nor is it a completely flat, immovable surface. Our therapeutic goal is a natural, relaxed look: to soften and diminish lines and furrows. And it is in this regard that we choose to use the term neuromodulation and not chemodenervation. It is about aesthetically choosing a therapeutic endpoint.10
 Mechanisms of Action
Mechanisms of Action
Botulinum toxin type A binds to the nerve endplate and blocks the release of acetylcholine. This bond is permanent and acetylcholine release begins again when the nerve sprouts a new endplate.11,12 The clinical effects after Botox injections begin in 3 to 5 days; the final effects are evident in 7 to 10 days and persist for 90 to 120 days. Our experience has been primarily with Botulinum toxin type A (Botox and Botox Cosmetic), but we have also used botulinum toxin type B (Myobloc) on occasion and have communicated with European physicians using Dysport. Myobloc has a more rapid onset of action than Botox (approximately 3–4 days), but also a shorter duration of action (∼42 days). Fifty to 100 units of Myobloc are equivalent to 1 unit of Botox.13,14 Dysport is also a type A botulinum toxin but has a more marked spreading effect and has a more complete ablation of dynamic rhytids. Patients have described its effect as “heavier” than Botox.15,16 Three to five units of Dysport are equivalent to 1 unit of Botox.17
 Relevant Facial Anatomy
Relevant Facial Anatomy
A thorough and intimate knowledge of facial anatomy is a prerequisite for understanding how to effectively employ neuromodulation as an adjunctive treatment in facial rejuvenation. Understanding the balance of facial musculature will allow the creative, effective, and safe use of this technique.18
The Forehead and Eyebrow
The broad, thin frontalis muscle elevates the forehead and eyebrows (Fig. 5-1). This muscle and the transverse forehead wrinkles that it can produce should be treated with great care and only in the appropriate patients. Patients who have blepharoptosis or redundant upper eyelid folds that impair the visual axis or constrict their peripheral visual fields will unconsciously elevate their eyebrows, attempting to expand their peripheral vision. These patients will notice transverse forehead furrows and often will want them treated. Treating their forehead furrows with neuromodulating agents can reduce their ability to raise their eyebrows and expand their visual fields and can also unmask or accentuate their blepharoptosis or eyelid heaviness. Our current concept is to modify the level and contour of the eyebrow by treating the brow depressors first and then treating any residual forehead rhytidosis during a subsequent treatment.

Figure 5-1 The broad, thin frontalis muscle elevates the forehead and eyebrow, and the orbicularis muscle depresses the eyebrow.
The corrugator, procerus, and orbicularis muscles are brow depressors. Treating them with neuromodulation can elevate the eyebrows, diminish upper lid heaviness, and reduce forehead furrows. Corrugator and procerus relaxation will elevate the medial and central brow. Relaxing the superior, lateral orbicularis muscle will elevate the lateral brow.19 These brow-elevating effects are best performed without treating the forehead itself. In this manner the frontalis can work to elevate the brow against the diminished activity of the brow depressors. Any residual forehead rhytidosis can be treated secondarily.
The Glabella
The powerful, paired corrugator muscles produce two deep vertical folds—the hallmark of intense frowning. At an early stage, neuromodulation can effectively relax these muscles and ablate these furrows. But when these muscles have been active for a long time and when the overlying skin has lost some of its turgor and elasticity, these furrows remain, even at rest. In these cases, combined filling and neuromodulation are necessary for a complete effect. The single, flat procerus muscle, when contracted, creates horizontal furrows on the bridge of the nose (Fig. 5-2). It can conveniently be treated with the corrugator muscles.
The Eyebrow and the Upper Eyelid
The position of the eyebrow will determine the degree of redundancy of the upper lid fold. An elevated eyebrow will lessen upper lid fold redundancy and a ptotic eyebrow will accentuate it. A ptotic eyebrow can even obscure the superior sulcus. In mild cases neuromodulation can postpone surgical correction of the upper lids and brows, demonstrate possible surgical outcomes, and diminish asymmetric surgical results. Treating the superior lateral portion of the orbicularis can effectively reduce crow’s feet and elevate the brow without risk of blepharoptosis. The eyebrow can be shaped with creative and intelligent neuromodulation. Treating the central portion of the superior orbicularis muscle will result in ptosis. This is often used effectively for temporary amelioration of corneal exposure and upper eyelid retraction.
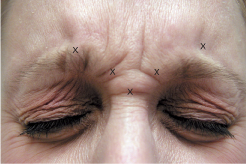
Figure 5-2 A hypertrophic, hyperactive corrugator muscle demonstrates prominent vertical furrowing and a broad insertion across the midline of the brow. A hypertrophic, hyperactive procerus muscle demonstrates marked horizontal furrowing of the glabella. Glabella injection sites (5.0 units per site) are noted.
The Lateral Canthus and Lower Eyelid
The inferior lateral portion of the orbicularis muscle can be treated lateral to the orbital rim to diminish crow’s feet without risk of displacement of the lower lid margin or change in the shape and dimensions of the palpebral aperture. Lower eyelid wrinkles and hypertrophic pretarsal orbicularis muscles (Fig. 5-3) can also be treated with neuromodulation provided that there is no lateral canthal or lower lid margin laxity. The lower lid pretarsal orbicularis can also be treated in younger patients wishing to widen their palpebral aperture. Completely eliminating a pretarsal orbicularis roll is not always indicated because it is considered to be a sign of youth. If there is preexisting laxity or lower lid retraction and the lower lid pretarsal orbicularis muscle is treated, lower lid retraction and inferior scleral show will be accentuated as will lower lid rhytidosis. This can be accompanied by premalar lymphedema. Aside from unmasking incipient lower lid laxity, neuromodulation of the lower lids may also reveal early lower lid fat herniation that the patient had not been previously aware of. This must be recognized, demonstrated, and explained to patients before they are injected.
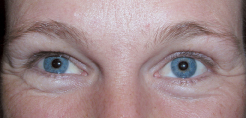
Figure 5-3 Hypertrophic, hyperactive pretarsal orbicularis oculi muscles create a transverse ridge on the lower lids. Patients may confuse these with lower lid “bags,” but these ridges are located more superiorly than prolapsed orbital fat. This patient exhibits a lower lid Botox effect on the left. There is less of a pretarsal orbicularis muscle fold and a widened vertical palpebral aperture.
The Orbicularis Oris, Depressor Oris Anguli, and Perioral Complex
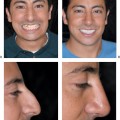
These muscles function in a delicate balance. The orbicularis oris functions as a sphincter. Its overaction can cause vertical upper lip rhytids. The depressor anguli oris muscle arises from the border of the mandible and inserts at the lateral corners of the mouth. This muscle contributes to the depth of oral commissure (melomental fold or marionette lines). Relaxing the depressor anguli oris allows the zygomaticus major and minor to elevate the corner of the mouth without opposition, facilitating filling of the oral commissures. But treating these areas requires precision. Misplaced or overdosed treatments can upset this delicate balance. Understanding this balance will allow the treating physicans to treat patients with facial asymmetries following Bell’s palsy (Figs. 5-4; 5-5A,B).

Figure 5-4 The perioral muscles are in delicate balance. The depressor anguli oris pulls the corner of the mouth down, while the zygomaticus major and minor pull it up.
The Platysma
This flat, broad muscle is also a lower lip depressor. It runs from the chin, at the oral commissures, to the deep subclavicular tissues. Neuromodulation of this muscle can assist in the amelioration of platysmal bands and concentric neck rings.20 Pretreatment of the platysma may also enhance the effects of facial tightening procedures like Therma-Lifting (Thermage, Hayward, California).

Figure 5-5 (A,B) In repose and animation, this patient exhibits upper and lower facial asymmetry, which was significantly improved with Botox neuromodulation.
 Clinical Applications
Clinical Applications
One hundred units of Botox Cosmetic powder are freeze-dried in each vacuum-sealed glass vial. Different vials can be mixed to different strengths for different muscles. Although it is apparent that, once reconstituted, Botox Cosmetic can remain active (if refrigerated) for several weeks, we are not certain if there is any degradation in potency during that time. We prefer to use our Botox within the first 4 hours of mixing it. There is also some discussion about the use of preserved saline versus nonpreserved saline. Although it is claimed that the use of preserved saline diminishes discomfort during injection (there is less of a burning sensation) and that it lengthens the time that reconstituted refrigerated Botox can last, we continue to use nonpreserved saline for reconstituting Botox. We feel that it may be more potent and gives reproducible results.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


