Nerve Repair and Reconstruction—Tibial Nerve
Shawn Moshrefi
Catherine Curtin
DEFINITION
Tibial nerve injuries can vary in severity, mechanism, and treatment.
Nerve injury categories1
Neurapraxia: conduction delay with no axonal injury. These injuries will recover spontaneously without intervention.
Axonotmesis: axonal injury resulting in disruption of the axons, but the supporting nerve scaffolding is intact. In these injuries, distal nerve segment will undergo Wallerian degeneration and proximal fibers will regenerate. Spontaneous recovery is possible.
Neurotmesis: complete disruption of the nerve. In these injuries, spontaneous regeneration will not occur.
Neuroma in continuity: disruption of the axons though the scaffolding seems to be intact. However, at the injury site, there is internal fibrosis, which prevents axons from regenerating. In these injuries, spontaneous regeneration will not occur.
Mixture of injury types: nerve patterns can be complex and one nerve can have several different types of injury.
ANATOMY (FIG 1)
Tibial nerve originates from L4 through S3 nerve roots.
The motor branches innervate the posterior calf compartment muscles and the majority of small muscles in the foot.
The sensory branches supply the knee joint, part of the sural nerve distribution, and the sole of the foot.
Tibial nerve branches from the sciatic nerve in the popliteal fossa.
The first branch off the tibial nerve is a sensory contribution to the sural nerve.
The next branches are the motor nerves to the gastrocnemius muscles.
Then, the tibial nerve passes through popliteal fossa under arch of soleus. (This area is a potential area of tibial nerve entrapment called the soleal sling.)
The tibial nerve courses distally adjacent to the tibia on undersurface of soleus in the leg running with the peroneal artery and vein.
At the ankle, tibial nerve is posterior to the medial malleolus adjacent to posterior tibial artery beneath the flexor retinaculum (This is a potential area of entrapment known as the tarsal tunnel.) (FIG 2).
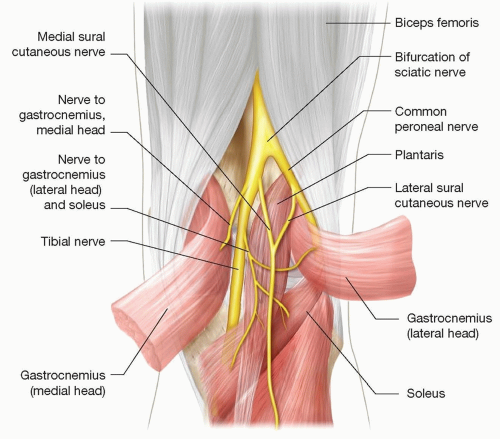
FIG 1 • Anatomy of the proximal tibial nerve.
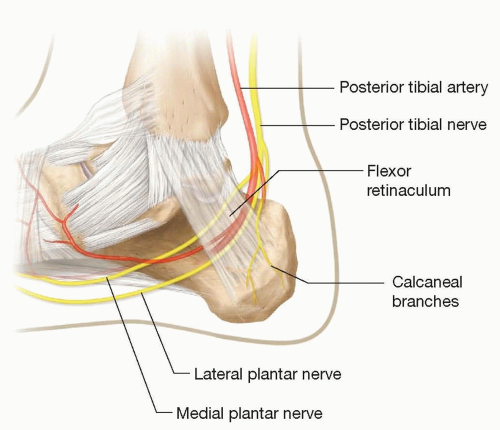
FIG 2 • Anatomy of the tarsal tunnel.
At the medial malleolus, the tibial nerve branches into the calcaneal, medial plantar, and lateral plantar nerves. The anatomy of the branching is highly variable between patients.2
PATHOGENESIS
Tibial nerves can be injured in many ways and in any location along its course. Listed below are some of the more common causes of tibial nerve injury.
Traumatic knee dislocation
Direct trauma to the popliteal area, both blunt or sharp
Iatrogenic prolonged tourniquet, hardware, or limb lengthening procedures
Ankle swelling or compression
Cysts or other nerve compressing structures (both in the popliteal fossa as well as at the medial malleolus)
PATIENT HISTORY AND PHYSICAL FINDINGS
A complete and thorough history detailing patient’s history of present illness, current injuries, history of prior injuries, prior surgeries (including spinal, buttock, and lower extremity procedures), comorbidities, occupation, and other case-by-case considerations should be obtained.
Inspection
Is the calf or foot swollen?
Are there vascular changes?
Is there atrophy?
Vascular exam—palpable pulses distally, temperature, and capillary refill of the toes and foot.
Sensory exam—Ten test: an area of normal or baseline sensation is compared to an area of concern for sensory loss and the difference is rated from 1 to 10 with 10 being the best score possible.3
Motor exam
Test the respective muscles that the tibial nerve and its branches supply (tibial nerve controls plantar flexion and inversion of the foot and ankle).
Each individual movement tested should be compared to the contralateral side. This allows the examiner to identify subtle weakness.
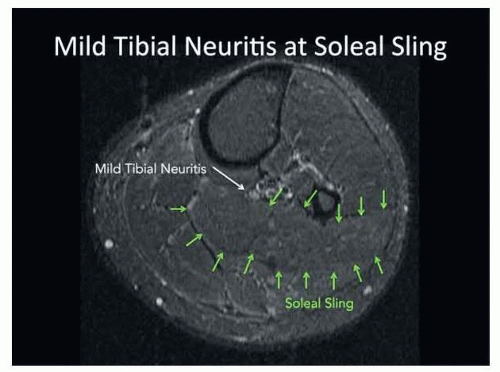
FIG 3 • MRI of tibial nerve at soleal sling. Note that the tibial nerve is bright like the surrounding vessels, and normal nerve is isointense with the muscle. (Courtesy of Sandip Biswal, Stanford University.)
Motor examination remember mnemonic TIP = Tibial Inverts and Plantar flexes.
Scratch collapse test.4 This tool originally described for the upper limb is also useful for assessing nerve entrapment in the lower limb. For this test, the examiner is testing external rotation of the arm.
To do this, the examiner has the patient sitting straight with arms adducted to their side and elbows bent to 90 degrees. The patient is told to keep the arm in this position.
The examiner then gently scratches the skin directly over the area of suspected nerve compression (eg, posterior to the medial malleolus for suspected tarsal tunnel).
After scratching the skin, the examiner then directly applies internal rotation force to the patient’s dorsal forearm while the patient actively attempts to resist. The test is positive for nerve pathology if the patient is briefly unable to resist your force of internal rotation.
Tinel sign
Point tenderness: the tibial nerve can be compressed at the level of the soleal sling. Patients are often tender to direct pressure over the site (posterior midline of the calf about 10 cm distal to the posterior knee crease).
IMAGING/STUDIES
X-rays are obtained if there is a suspected bony injury.
MRI can assess for soft tissue masses such as Baker cysts and also provide information on the nerve.
Enhancement of fascicles on MRI can help identify tibial neuritis (FIG 3).Related posts:
 Fasciotomy of the Thigh, Lower Leg, and Foot
Fasciotomy of the Thigh, Lower Leg, and Foot
 Bony Reconstruction of Foot and Ankle (Bone Grafts)
Bony Reconstruction of Foot and Ankle (Bone Grafts)
 Vascular Reconstruction of Lower Extremity, Foot, and Ankle
Vascular Reconstruction of Lower Extremity, Foot, and Ankle
 Tibial Reconstruction
Tibial Reconstruction
 Reconstruction of Femur
Reconstruction of Femur
 Amputation of the Lower Extremity: Above-Knee Amputation, Below-Knee Amputation, Through-Knee Amputation
Amputation of the Lower Extremity: Above-Knee Amputation, Below-Knee Amputation, Through-Knee Amputation

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


