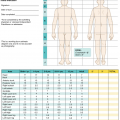
Classification
Type of lesions
Distribution
%BSA
EMM
Typical target
Acral
–
SJS
Spots atypical target
Widespread
<10
SJS–TEN overlap
Spots atypical target
Widespread
10–30%
TEN with spots
Spots atypical target
Widespread
≥30%
TEN without spots
Diffuse erythema, no spots or target
Widespread
≥30%
43.2 Epidemiology
The incidence is 2–7 cases per million people per year [3]. It is well known that this rare drug reaction affects women at a slightly higher rate than men. SJS/TEN can occur at any age group, but it appears to affect adults more than children [4]. Mortality rates of SJS, SJS-TEN, and TEN were 5–10%, 30%, and 50%, respectively [5, 6].
HLA association in different population
Associated drug | HLA allele | Specific eruption | Ethnicity |
|---|---|---|---|
Aromatic convulsant | B∗15:02 | SJS/TEN | Han Chinese, Indian, Malaysian, Vietnamese, Singaporean, Hong Kongese |
Carbamazepine | A∗31:01 | DRESS/SJS/TEN | Northern European, Japanese, Korean |
B∗15:11 | SJS/TEN | Han Chinese, Japanese, Korean | |
B∗59:01 | SJS/TEN | Japanese | |
B∗38:01 | SJS/TEN | Spanish | |
B∗15:02 | SJS/TEN | Han Chinese, Thai | |
B∗51:01 | SJS/TEN | Han Chinese, Japanese, Malaysian | |
Oxcarbazepine | A∗33:03, B∗38:02, B∗51:01, B∗56:02, B∗58:01, C∗14:02 | SJS/TEN | Thai |
Phenytoin | B∗15:13 | DRESS/SJS/TEN | Malaysian |
CYP2C9∗3 | DRESS/SJS/TEN | Han Chinese, Japanese, Malaysian | |
CYP2C9∗3 | SJS/TEN | Thai | |
B∗15:02 | SJS/TEN | Han Chinese | |
B∗38; B∗58:01, A∗68:01, Cw∗07:18 | SJS/TEN | European | |
Phenobarbital | B∗38:01 | SJS/TEN | Spanish |
Lamotrigine | A∗31:01 | SJS/TEN | Korean |
A∗24:02 | DRESS/SJS/TEN | Spanish | |
Allopurinol | B∗58:01 | DRESS/SJS/TEN | Han Chinese, Thai, Japanese, Korean, European |
Nevirapine | C∗04:01 | DRESS/SJS/TEN | Malawian |
Cotrimoxazole | B∗15:02, C∗06:02, C∗08:01 | SJS/TEN | Thai |
Sulfamethoxazole | B∗38:02 | SJS/TEN | European |
Sulfonamide | A∗29, B∗12, DR∗7 | TEN | European |
Oxicam NSAIDs | B∗73:01 | SJS/TEN | European |
Methazolamide | B∗59:01, CW∗01:02 | SJS/TEN | Korean, Japanese |
Use of medication is the most common cause of EN. Other rare causes reported in literature include infection and vaccination, and collagen vascular diseases have been found to account for a small number of cases [10–13]. This is most likely due to confusion regarding diagnostic consideration among SJS, EM, and Mycoplasma pneumoniae-induced rash and mucositis (MIRM).
High-risk drug causing epidermal necrolysis
Allopurinol Aromatic anticonvulsants: carbamazepine, phenobarbital, phenytoin Antibacterial sulfonamides: sulfamethoxazole, sulfasalazine Lamotrigine Nevirapine Oxicam nonsteroidal anti-inflammatory drugs |
43.3 Pathogenesis
Several theories have been proposed for the pathogenesis of epidermolytic necrolysis, but molecular sequencing and cellular events are not fully understood. In susceptible individuals, upon exposure to a certain drug or one of its metabolite, a series of reactions occur that lead to keratinocytes apoptosis and subsequent epidermal necrosis and detachment [9].
43.3.1 Antigen Presentation
Drugs are considered as foreign body material that are too small on their own to be immunogenic. But when they bind to hapten-carrier complex, they are presented to HLA molecules, and then are recognized by T-cell receptors (TCR). This recognition results in the induction of drug-specific immune response by CD8+ cytotoxic T cell (CTL).
43.3.2 Fas-FasL Interaction
Fas ligands (FasL) are transmembrane protein molecules expressed on target cells that belong to tumor necrosis factor (TNF) family. Upon their interaction, Fas-associated death domain proteins (FAAD) is recruited and bind to Fas-FasL complex. Subsequently, FAAD recruits procaspase 8, turning it into caspase 8 and triggering it into caspase cascade which result in DNA degranulation. However, the molecular events leading to the upregulation of surface keratinocyte FasL during TEN remain unknown [17].
43.3.3 Perforin/Granzyme B
Other research suggests that perforin and granzyme B play more important role in keratinocytes apoptosis in EN than does Fas–FasL interaction. Granzyme B is a serine protease released by cytoplasmic granules that induce apoptosis. Upon activation, CTL and natural killer cells (NK) produce perforin, which in turn delineates the entry of granzyme B into the target cells [18–20].
43.3.4 Granulysin
Granulysin is a cytolytic protein produced mainly by CTL, NK cells, and NK T cells. This molecule participates in programmed cellular death by creating holes in cellular membrane and thereby cellular destruction. In 2008, Chung et al. provided evidence that granulysin is the key mediator for disseminated keratinocyte apoptosis in SJS/TEN. This study found that the granulysin level in blister fluids of SJS/TEN patient was much higher than other cytotoxic proteins, such as Fas-FasL, perforin, and granzyme B [21].
43.3.5 Delayed-Type Drug Hypersensitivity
Specific T lymphocytes or NK cells are activated upon antigen recognition. Soon afterwards, various cytokines/chemokines are released to attack keratinocytes or promote trafficking, proliferation, regulation, or activation of T cells and other leukocytes.
43.3.6 Other Cytokines and Chemokines Are Involved in EN Pathogenesis Such as TNF-α, IFN-γ and IL-15 & IL-36
TNF-α is a major proinflammatory cytokine and is produced by macrophages, T lymphocytes, NK cells, neutrophils, mast cells and eosinophils. This molecule is highly expressed in plasma and blister fluids of SJS/TEN and appear to be a significant inducer of keratinocyte apoptosis [22].
IFN-γ is a significant cytokine for innate and adaptive immunity that is mainly produced by CD4+ T-helper cells, CD8+ CTL, and NK cells. IFN-γ was found to be elevated in skin tissue, blister, and plasma of SJS/TEN patients. In 2013, Viard-Leveugle et al. suggested a link between two path mechanism modalities of EN, delayed-type drug hypersensitivity and target cellular death. This study demonstrated that activated T cells secrete high amount of TNF-α and IFN-γ which lead to an increased expression and activity of inducible nitric oxide synthetase (iNOS). The resulting increase in nitric oxide significantly upregulates keratinocyte FasL expression and eventually keratinocyte apoptosis.
IL-15 and IL-36 participate in the immune reaction of EN by regulating trafficking, proliferation, and activation of T lymphocytes. Moreover, IL-15 has also been shown to enhance the cytotoxicity of cultured NK cells and blister cells from TEN [5]. Thereby IL-15 has been found to be associated with disease severity and mortality of SJS/TEN.
43.4 Clinical Presentation

Related posts:
 of Burn Patients to the Burn Center Including Burn Wound Evaluation
of Burn Patients to the Burn Center Including Burn Wound Evaluation
 Care of the Burned Patient
Care of the Burned Patient
 Management of Facial Burns, Acute Versus Long-Term, Surgical Versus Non-surgical Face Transplant
Management of Facial Burns, Acute Versus Long-Term, Surgical Versus Non-surgical Face Transplant
 Management of Burn Patients and Fluid Resuscitation
Management of Burn Patients and Fluid Resuscitation
 Improvement in Burn Care
Improvement in Burn Care
 Reconstruction: The Role of Integra in the Dorsum Hand and Wrist Reconstruction
Reconstruction: The Role of Integra in the Dorsum Hand and Wrist Reconstruction
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


