Key points
- •
Indications include young patients with a prematurely aged neck, or patients with the neck as a prominent aspect of facial aging.
- •
Treatment of the platysmal laxity may bring about a more youthful cervicomental angle.
- •
Submental fullness may be addressed with conservative contouring of subplatysmal fat.
- •
Fat grafting in selected areas along the mandibular border, chin and submental area may significantly enhance the appearance of the lower face and neck
- •
Fullness laterally below the mandible may be the result of the ptotic submandibular gland and is addressed via gland resection or suspension.
- •
Aesthetic facial surgical procedures that do not address the neck may otherwise accentuate the cervical laxity, but rhytidectomy paired with necklift can have dramatic rejuventative effects.
Introduction and etiology
The progressive development of soft-tissue laxity, excess, deflation and ptosis combine to convey the appearance of premature aging in the neck. A properly defined cervicomandibular angle is a key element of facial harmony and contributes to a more youthful appearance of the head and neck. Rejuvenation of the aging neck gives a more pleasing appearance to the soft tissues in that area, and can cause the face to appear more youthful as well. Guerrerosantos discussed the necklift in 1983. There have been numerous additions and refinements to his approach, and the idea has steadily gained popularity. As a result, rejuvenative procedures of the cervicofacial region are among the most commonly performed cosmetic surgical procedures in the United States.
The mechanism of the aging process in the face and neck is not well understood. Aging of the soft tissues of the face and neck was thought to be due to ptosis of the skin resulting from the effect of gravity and many surgeons felt that underlying structures played a minor role, if any in this process. However, anteroposterior changes in volume can lead to the false appearance of skin descent ( ). Lambros described this volume-loss theory of facial aging which we feel is valid.
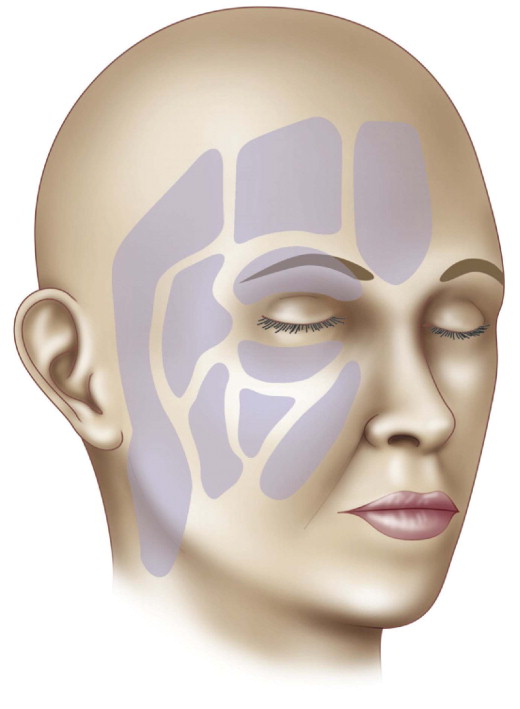
New evidence indicates that volume loss in the subcutaneous fat layers may play a larger role than previously thought. Rohrich and Pessa recently characterized the subcutaneous fat compartments of the face and postulated that these compartments are differentially affected by facial aging ( ) ( Figure 8.1 ). Descent of facial soft tissues proceeds inferiorly and inferomedially. Rejuvenation involves repositioning the tissue in superior and supero-lateral vectors ( ). The senior author’s technique addresses the various tissues responsible for premature aging in the neck, corrects discrepancies in volume, and repositions them in the correct vectors ( ). Several approaches have evolved to include minimally invasive techniques to correct the aging neck ( , ), however, our recent work also effectively addresses discrepancies in the volume of both fat and glandular tissues in the prematurely aged neck, while repositioning tissues in the correct vectors. We also feel the appropriate addition and removal of fat along the jaw line and in the neck is extremely helpful in certain facial types.
Anatomy and effects of aging
Several elements define the aesthetic cervicofacial region, as defined by Ellenbogen as early as 1980. Smooth skin surfaces drape cleanly over the deeper structures of the neck, without rhytides or obvious laxity. Ideally, the cervicomental angle falls between 90 and 105 degrees. Patel et al present a comprehensive review of the anatomy of the neck relevant to necklift ( ). The two rays that compose this angle are the almost horizontal submandibular plane and the more vertical aspect of the anterior neck. The union of these rays corresponds with the skin landmarks overlying the anterior surface of the hyoid. These skin surfaces which compose the cervicomental angle drape over a variety of deep structures. An accurate understanding of these structures, and how they change with aging, is paramount to undertaking rejuvenation of the neck. The horizontal ray of the cervicomental angle comprises, from shallow to deep: skin, subcutaneous fat, the platysma (Greek: ‘plate’), subplatysmal fat, the anterior bellies of the digastric muscles, the border of the mandible, and the submandibular glands. The vertical ray of the cervicomental angle is composed of the following structures, again from superficial to deep: skin, subcutaneous fat, the platysma, subplatysmal fat, the strap muscles of the neck, the thyroid and its cartilage, and the tracheal cartilages.
In youth, the gentle outlines of the thyroid cartilage are visible, as are the anterior borders of the sternocleidomastoid muscles. A small concavity is present at the junction of the origins of the sternocleidomastoid muscles, as the suprasternal notch. The platysma has sufficient tone to provide an even, smooth layer which closely invests the thyroid cartilage, hyoid, and sub-mental soft tissues. It is essentially an extension of the superficial musculoaponeurotic system (SMAS). Retaining ligaments in the neck, analogous to those in the face, tether the skin to the anterior aspect of the inferior mandibular border and platysma.
The skin overlying the mandible should be of sufficient tone so it closely invests the mandibular border. The submandibular glands should be palpable beneath the mandibular border but should be maintained by their ligamentous attachments in a position such that they are tucked deep to the mandible. These glands should not be enlarged or ptotic to the extent that they cause visible bulges in the overlying soft tissues. Depressions from the perioral tissues to the mental area should not be present. These labiomental rhytides are best addressed by facelift procedures, which are often an effective adjunct to neck rejuvenation.
Signs of the prematurely aged neck are manifest in several stages. Often, the earliest indication of cervicofacial aging is the gradual development of faint vertical bands in the platysma muscle superficial to the thyroid cartilage and hyoid bone. These platysmal bands progress to longer, more apparent, slips of tissue as more support is lost from the retaining ligaments and the platysma descends further ( ). The platysmal muscle fibers may dehisce and lose mechanical advantage over the slackening soft tissues of the neck, further increasing the cervicomental angle. This phenomenon is best demonstrated with voluntary facial grimacing. The combination of platysmal laxity and pre- and subplatysmal fat deposits exacerbates the evolving cervical obliquity. Matarasso et al proposed a classification system (I to IV) based on horizontal neck rhytids, platysma bands, and skin laxity. These classifications correlated with the degree of age-related neck degeneration ( ).
Laxity of the suspensory tissues, descent of deeper structures, and fat deposits combine to form the stigmata of premature aging in the neck. Descent of the jowls may contribute to the loss of definition of the inferior mandibular border. Submandibular gland ptosis conveys the effect of greater bulk laterally, below the angle of the mandible. Conversely, the bone mass of the mandible tends to resorb over time, which serves to worsen the descent of the soft-tissues of the chin and neck. Deflation also takes place in the pre-jowl sulcus and over the angle of the mandible. The progressive descent and volume discrepancy contribute to cervical fullness, and the end result of all of these processes is a neck with a prematurely aged appearance.
Occasionally, pre-existing micro- or retrogenia compounds the aged appearance of the neck. Some believe that chin augmentation or chin advancement in these cases helps rejuvenate the soft tissues of the chin and neck and contributes to a more appealing result ( ). However, we prefer the use of fat grafting to the anterior aspect of the chin to supplement the mental fat pad.
Patient selection
The key to obtaining a result in neck contouring procedures is pairing the correct procedure, in the correct measure, to the patient. We have found enormous variability between individual neck types. Therefore, pre-operative evaluation, a focused history and physical examination, and standardized photographs are vital in outlining any approach to neck rejuvenation. Matching the patient’s concerns and expectations with the surgeon’s skills and with obtainable results is paramount. It is also important to keep in mind what effect redraping and resuspending certain tissues will have on the nearby structures. For example, a procedure to tighten the platysma may not address the jowls, and a rejuvenated neck may accentuate the effects of aging in the lower and midface. It is the surgeon’s responsibility to foresee and address these conflicts preoperatively, in order to ensure a well-designed treatment plan, which provides the most aesthetic result for the patient.
Indications
Indications include young patients with a prematurely aged neck, those with a greater degree of subplatysmal fat deposits than expected for their body habitus, or patients with the neck as a prominent aspect of facial aging. Other indications include those patients undergoing other aesthetic facial surgical procedures which otherwise accentuate the neck laxity. Contraindications are similar to those for other elective aesthetic procedures such as those with bleeding disorders, wound healing problems and medically high-risk patients, etc. As always, a thorough history and focused physical examination with discussion of the patient’s desired change in their appearance is essential. Patients with unrealistic expectations of the surgical outcome are not considered surgical candidates.
Operative technique
Pre-operative preparation
Intravenous sedation without intubation, paralytic drugs, or general anesthesia has been our anesthesia treatment of choice for over a decade ( ). Local anesthesia in the form of lidocaine or bupivacaine mixed with epinephrine is also administered using the lowest concentration possible. Our nerve blocks are performed with bupivacaine. If submandibular gland suspension is planned our standard protocol includes a thorough betadine prep of the oral cavity followed by intra-oral administration of local anesthesia to block the area.
Surgical exposure to the neck is gained through an inconspicuous 3.5 cm submental incision in the shadow posterior to the submental skin crease. This allows access to the platysmal plane. Laterally, the neck is approached through a conventional pre- and posterior auricular rhytidectomy incision. This gives good visualization along the inferior border of the mandible, and provides an avenue for directly visualized suction lipectomy of the neck. A short scar technique is our preference. Occipital incisions are avoided when possible, as they may be more apparent when patients wear their hairstyle short or pulled in a tight ponytail ( ). We do extensively utilize the post-auricular crease as it provides additional exposure and removal and redraping of excessive skin. Feldman advocates the use of 1.5 inch ‘helper’ incisions in the retroauricular area, to assist in undermining the lateral neck and as exit insions for lateral suction drains ( ). However, we have a small drain exit superior and posterior to the incision in an effort to produce a perfectly smooth skin closure.
Technique
SMAS suspension/platysmal plication
Rhytidectomy in conjunction with a neck lift can provide further suspension of the soft tissues of the lateral neck. This is accomplished by the changed vector that results from the transposition of a vertical strip of preauricular SMAS to an anchor point in the retroauricular area. The lift is thereby changed from a vertical one to a more attractive line below the angle of the mandible.
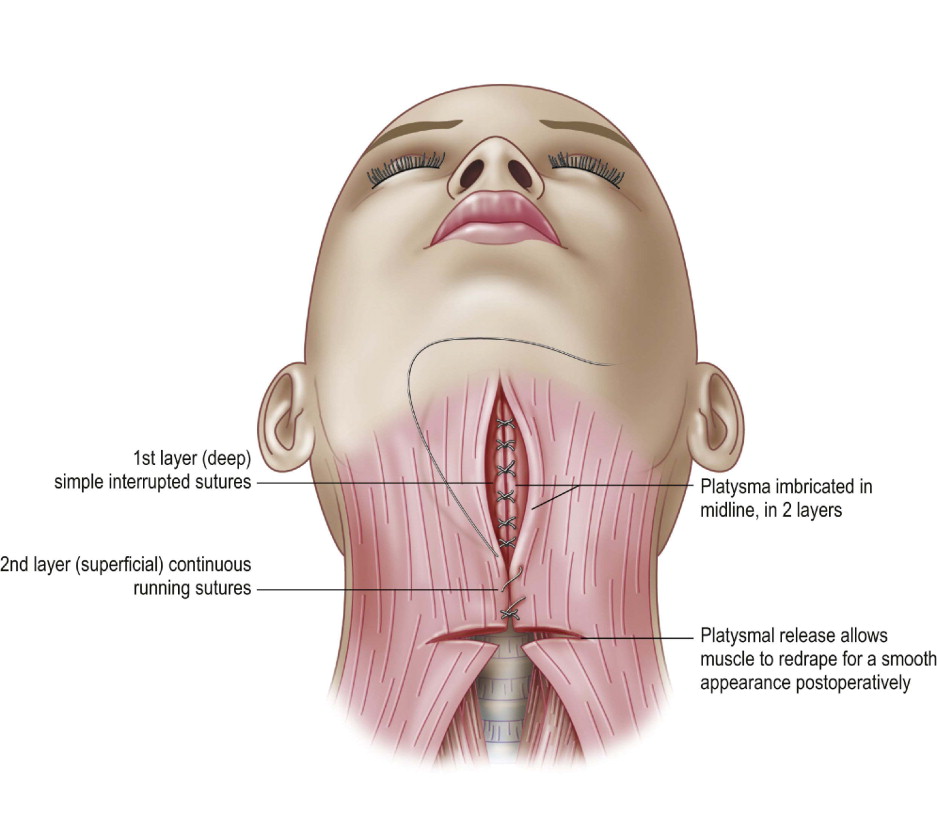
The goal in platysmal plication is to provide an even, smooth platysmal layer which closely invests the thyroid cartilage, hyoid, and floor of the mouth. The anterior platysma is best approached by means of a transverse submental incision ( Figure 8.2 ). The skin is then undermined inferiorly at least to the level of the cricoid. To adequately correct the effects of platysmal banding, the edges of the muscle are freed from the deeper subplatysmal fat and the digastric anterior muscle bellies. The edges of the platysma are grasped and brought to the midline. Any excess tissue is then contoured down and resected, the edges approximated accordingly, with a series of interrupted sutures followed by a running suture the full length of the closure.