Summary
Accurate determination of the nature of the defect is essential in anatomic-based reconstruction planning.
In reality, a few basic techniques will manage a majority of defects.
Complex defects most often require a paramidline forehead flap for reconstruction.
14.1 Algorithm for Closure (▶ Fig. 14.1)
14.1.1 Sidewall
The sidewall is frequently involved with skin cancer and can often be simply closed as a linear incision. Larger defects may require a non-subunit, color-matched full-thickness skin graft or nasolabial flap (▶ Fig. 14.3, ▶ Fig. 14.4, ▶ Fig. 14.5).
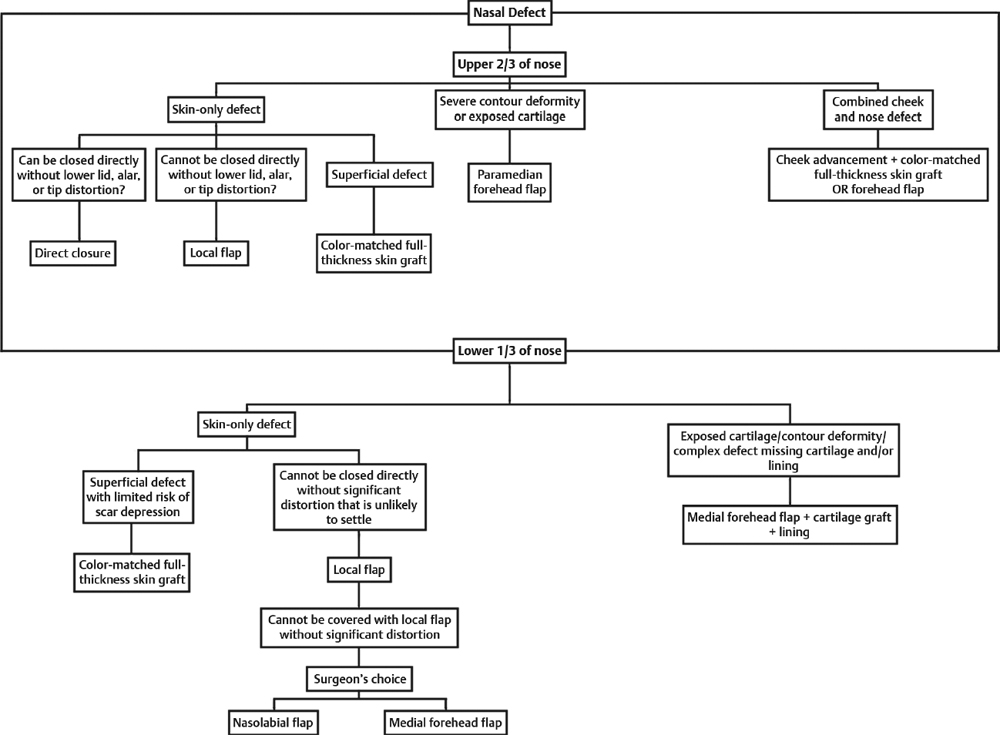
Fig. 14.1 Algorithm for closure of defects on the upper two-thirds versus lower one-third of the nose.
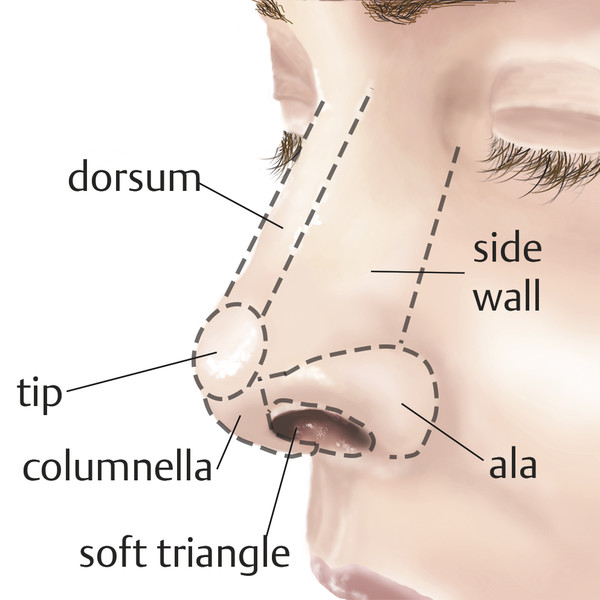
Fig. 14.2 Nasal subunit anatomy.

Fig. 14.3 A 60-year-old male status post Mohs excision for basal cell carcinoma at left nasal sidewall. Defect-only reconstruction with primary closure and standing cone excision. Postoperative results show at 5 months. Although this is an exaggerated example, the patient’s inherent laxity allowed undermining and significant closure with meticulous extension of the standing cones, one of which extended into the anterior ala subunit.
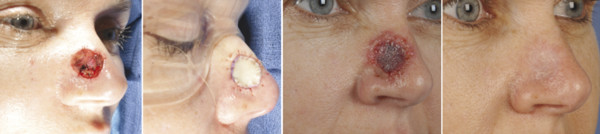
Fig. 14.4 A 49-year-old female status post 1 × 2 cm Mohs excision of basal cell carcinoma on right nasal sidewall. Defect-only reconstruction with color-matched full-thickness skin graft from preauricular donor site. Postoperative results shown at 1 week and 6 months.

Fig. 14.5 A 63-year-old female status post Mohs excision for basal cell carcinoma as nasal side wall. Defect-only reconstruction with nasolabial flap. Postoperative results shown at 1 year.
Dorsum
Cephalic dorsal defects can also be frequently managed with simple vertical closure, often with wide undermining. For patients with thin skin non-subunit, full-thickness skin grafting is ideal. For defects with exposed cartilage or significant contour deformity, a nasolabial flap or a paramidline forehead flap is predictable and ideal 1 (▶ Fig. 14.6, ▶ Fig. 14.7, ▶ Fig. 14.8, ▶ Fig. 14.9).

Fig. 14.6 A 49-year-old male status post Mohs excision for basal cell carcinoma at nasal dorsum. Defect-only reconstruction with direct vertical closure. Postoperative results shown at 1 week and 1 month.

Fig. 14.7 A 45-year-old female status post 1 × 2 cm Mohs excision for basal cell carcinoma on medial dorsum of nose. Defect-only reconstruction with color-matched full-thickness skin graft from preauricular donor site. Postoperative results shown at 2 and 4 months from left to right.

Fig. 14.8 A 66-year-old female status post Mohs excision of basal cell carcinoma at nasal tip. Defect-only reconstruction with nasolabial flap. Final results shown at 7 months.

Fig. 14.9 A 77-year-old male status post 3 × 2 cm Mohs excision for squamous cell carcinoma at nasal dorsum. Defect-only reconstruction with paramidline forehead flap. Postoperative results shown in bottom row at 5 weeks, 5 months, and 2 years.
Combined Cheek and Nasal Sidewall
These are common defects and frequently mismanaged by simply “dragging” the cheek skin up to close the cheek and nasal defects; this completely disrupts the cheek–nose junction and is unsatisfactory. The correct approach is to manage the two individual anatomic defects; first the cheek is advanced and closed, often without undermining. When the cheek–nose junction is restored based on the normal contralateral side, the nasal sidewall defect is managed. For relatively shallow defects, simple color-matched full-thickness skin grafting is performed—often the skin can be obtained from the discarded standing cones on the cheek advancement flap. Thicker defects with exposed bone and cartilage are treated with either a turnover flap and full-thickness skin graft or a concurrent paramedian forehead flap 2 (▶ Fig. 14.10, ▶ Fig. 14.11, ▶ Fig. 14.12).
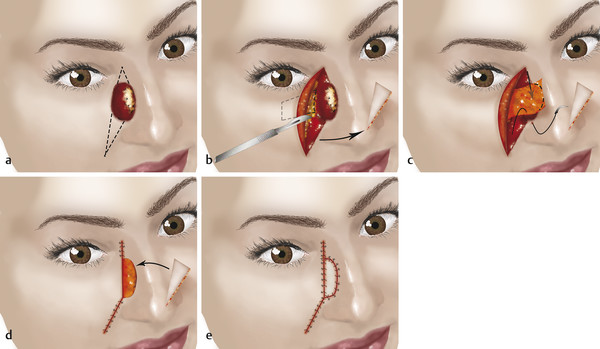
Fig. 14.10 (a) Combined cheek and nasal defect with exposed nasal bone and cartilage. Dog-ear excisions for plain cheek advancement flap drawn; (b) cheek advancement flap elevated with soft-tissue turnover for nasal side wall designed and dog-ear excision remnant saved; (c) soft-tissue flap rotated and inset to cover nasal bony defect; (d) cheek advanced and inset; (e) dog-ear excision remnant trimmed and inset as full-thickness nasal side wall graft.

Fig. 14.11 A 63-year-old female status post 3 × 2 cm Mohs excision for squamous cell carcinoma involving medial cheek, lower eyelid, and nasal sidewall. Defect-only reconstruction with cheek advancement flap and turnover soft-tissue flap with simultaneous full-thickness skin graft at nasal sidewall. Skin graft harvested from stand cone excision tissue. Postoperative results shown at 1 month.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


