Summary
There are two flaps most applicable to complex nasal defects—the nasolabial flap and the forehead flap.
Only the forehead flap can provide enough robust tissue to reliably treat lining defects.
Generally both flaps are done as two or more staged procedures.
13.1 General Principles in Complex Nasal Defects and Reconstruction
Complex nasal repairs include larger coverage-only defects, defects involving multiple subunits, or defects with missing cartilage and lining.
The fourth category of general techniques in nasal reconstruction is the use of nasolabial and forehead flaps. Both techniques allow the predictable transfer of large volumes of well-vascularized color-matched tissue. Generally, both flaps are performed as two or more staged procedures. Despite proper execution of the nasolabial flap, it has inherent design flaws that include marginal vascularity and irreversible donor-site contour deformity that the forehead flap does not have. Additionally, the forehead flap is able to provide lining and any volume of coverage needed, while the nasolabial flap is limited in size and is unable to provide reliable lining. 1
13.1.1 Nasolabial Flaps
The nasolabial flap is based on the utilization of redundant skin over the nasolabial fold. This implies that the patient does in fact have a nasolabial fold with redundant skin and for this reason the flap is often not successful if utilized on patients without well-defined cheek laxity and a well-defined nasolabial fold. 2 The nasolabial interpolation flap can be based inferiorly or superiorly with superior-based flap being the most useful. Superiorly based nasolabial flaps receive their blood supply via the angular artery, as it connects to the anterior facial artery and to the dorsal branch of the ophthalmic artery. 3 The nasolabial interpolation flap has been classically described for alar-only defects, but has shown to be quite useful for alar, tip, nasal sidewall, as well as nasal dorsum defects. 4
There is no doubt that any clinical surgeon can find fault with the final aesthetic result of a nasolabial flap, namely, the effacement of the cheek contour and resulting cheek asymmetry that is not often corrected. That being said, it can be a useful adjunct for nasal reconstruction in patients who will not tolerate a forehead flap or the degree of the defect does not mandate the surgical intervention of a forehead flap. 5 The nasolabial flap is most useful in smaller defects, posteriorly based alar defects, and defects in patients who medically, personally, or aesthetically will not tolerate a forehead flap. It is very important not to confuse the indications for the nasolabial flap with the forehead flap. The skin supply, volume of tissue provided, the skin type, the appropriate predictably, and final aesthetic results from a nasolabial flap are far less than the results provided with forehead flaps and they should not be considered interchangeable. Additionally, although described by other authors, our experience with nasolabial flaps is that they are not useful for defects that require lining reconstruction. Additionally, a subcutaneous island pedicle nasolabial flap has limited application in clinical practice, given the poor cheek appearance and sometimes the ultimately poor nasal appearance. 6 Rather, the procedure is performed with an interpolation flap which allows the practicing surgeon to perform a final “fine tuning of the nasal defect repair” at the time of division and insert. 5
The described version of the nasolabial flap is simply a superiorly based interpolation flap based on the perforators from the angular artery. It is a random pattern, not axial pattern, and again requires redundant cheek skin. The flap is elevated with the inferior aspect of the incision based on the nasolabial fold with distal extension directly adjacent to the lateral commissure of the lip. Properly closed, the cheek scar will heal well. Although this is a random pattern flap, it is robust, able to be elevated, and can reach significant distances that greatly exceed the normal 3:1 ratio (length:width ratio) of random pattern flaps. With proper flap design, the flap can easily reach the nasal tip and for patients with nasal tip defects when paramidline forehead flap is contraindicated, a nasolabial flap can provide a robust reliable nasal tip reconstruction. 5 Interpolated nasolabial flaps are routinely performed under intravenous sedation or local anesthetic only. The flap is elevated sharply with blunt medial dissection and rotated medially for inset. For all defects except the ala, the flap is inset under a slight amount of tension. The entire flap is covered with nitropaste and then is wrapped in fibrillar collagen for postoperative hemostasis. 7 The dressing is simply washed off in the shower by the patient on the third postoperative day. At that point, no further dressings are required and the flap can be simply covered with antibiotic ointment only. The flap is divided at no less than 3 weeks and at the time of division, no attempt is made to save any of the flap pedicle remnants. It is excised directly and then closed as a straight incision. Primary dermabrasion is performed on the flap scar within the nasolabial crease as well as its location on the nose at the time of inset. 8 The reconstructed nasal portion is elevated at least over 60% of its maximal volume, contoured, and inset. The flap is useful for total alar defects, nasal sidewall defects, and nasal dorsum defects. For sidewall and dorsum defects, the flap is significantly thinned and inset under slight tension. For nasal tip defects, the flap is thinned only to match the volume of the existing nasal tip contour. No attempt is made to perform subunit reconstructions for nasal tip defects with the nasolabial flap and this will only contribute to the poor donor-site appearance and will not provide a significant improvement over a defect-only reconstruction of the nasal tip. Special mention is made of the use of cartilage grafting. It is routinely used in alar contour grafts which can often be small partial-thickness conchal bowl incision routinely used for nasal defects within 7 mm of the alar rim. Special note is made of the soft triangle defect. This is a common defect and it is critical that this area is reconstructed to maintain the alar nasal angle. Isolated soft triangle defects are preferentially repaired with a nasolabial flap with a nonanatomic alar contour graft. The graft can be significantly thinned in contour and sewn in place for the small and often difficult to reconstruct defects (▶ Fig. 13.1).

Fig. 13.1 (a) The vertical dimensions of the nasal defect are transposed to the nasolabial fold on the cheek. Adequate flap length is confirmed with the reverse Gilles test. The flap is elevated lateral to medial, initially sharply and then bluntly as the perforating vessels are approached. The flap is inset under slight tension. (b) The flap is divided at no less than 3 weeks and when soft-tissue edema has resolved. The donor pedicle on the cheek is sharply excised and discarded and the incision closed directly. The inset portion of the flap on the nose is elevated over at least 60% of its volume and inset under slight tension.
13.1.2 Forehead Flaps
The previous discussion in nasal reconstruction has covered techniques available for soft-tissue coverage only. There are three distinct requirements for successful nasal reconstruction, namely, coverage, lining, and support, and the previous descriptions all assumed adequate lining and intact cartilage framework. For defects that require reconstruction of all three—coverage, lining, and cartilaginous support—there is only one reliable option: the paramidline forehead flap, with cartilage grafting if required. Additionally, the usefulness of the paramidline forehead flap for coverage-only defects is unparalleled with its ability to bring in large volumes of well-vascularized soft tissue with ideal color match. Understandably, there are significant short-term morbidities. The postoperative care is extensive. It is not a popular flap for a patient to have and the difficulty in patients who require eyeglass wear is also understood.
As was briefly discussed at the beginning of this section on nasal reconstruction, it is understood that the few and real masters currently practicing nasal reconstruction rely on less than a handful of surgical techniques and all large nasal reconstructions are performed using a paramidline forehead flap. Any surgeon who is looking to develop world-class results would do well to utilize the forehead flap more.
There are numerous forehead flap pedicle designs. These include the up-down flap, the ipsilateral or contralateral axial pattern flap, the “Dallas design” or paramedian contralateral flap, the median forehead flap, as well as the transverse or oblique forehead flap. In recent review of over 400 forehead flap cases with utilization of a multitude of forehead flap designs, several principles of flap design are true and can serve as guiding principles for flap design.
Maintenance of an axial pattern arterial pedicle greatly increases the reliability and versatility of the flap.
By utilizing the flap design ipsilateral to the defect, the axial pattern vascularity is maintained, as well as the provision for a secondary flap harvest in the event that this is required. The use of reasonably narrow pedicle based on Doppler identification of the artery will help in both minimizing the forehead flap donor-site scar and allowing for a lax easy rotation.
Early subperiosteal dissection will capture the periosteal blood supply to the flap and is easily performed at the level of the brow with acceptable postoperative donor site.
Meticulous attention to forehead flap closure prior to flap inset.
It is preferable to perform the initial forehead flap itself under a general anesthetic to assess the viability of the flap as well as for patient comfort. Patients who are candidates for safe general anesthesia are uniformly candidates for forehead flap reconstructions. Careful examination of the forehead with regard to previous surgical incisions or previous surgical scars is made, as well as assessment of the vertical height of the forehead and the volume of the forehead skin available in comparison to the volume requirement of the defect. Intraoperatively, the patient is placed supine and the bed rotated 180 degrees. The patient is placed in a slight reversed Trendelenburg position to decrease venous bleeding. The eyes are prepped into the field with lubricant and the neck is also prepped into the field if a full-thickness graft is required. Although the vascular pedicle for paramedian forehead flap is reliably located based on anatomic landmarks (1.7 cm from the midline), it is preferable to actually Doppler the pedicle at the level of the eyebrow, mark it and then center with calipers the flap width directly over the identified axial pattern vessels. This allows for more safety and flap elevation and comfortable application of Bovie cautery during the flap elevation. The template for the surface markings of the flap is preferably made from the contralateral nose. Initially, all the subunits of the nose are marked on the normal side. The decision is made regarding whether a subunit (preferable) or defect-only reconstruction is to be made and then a very accurate foil pattern or Steri-Stripped pattern that accurately corresponds to the three-dimensional surface area of the defect is made and transposed to a foil template. The soft lead foil wrappers of wine bottle cork covers can also be used as a template, given that this conforms very accurately to the contralateral side. Additional items have been described, including heat soluble thermoplast and neurosurgical bone wax to recreate an accurate template. Once the template has been accurately outlined and made and transposed to the contralateral side or reversed to allow accurate size matching on the opposite side, then it is transposed to the forehead. As a rule, a 1.5-cm pedicle is utilized with the tendency for a wider pedicle in active smokers. Every attempt is made to avoid transposing the flap into the hairline. 9 Carrying hair-bearing skin down to the flap is a significant postoperative morbidity for all patients and, no matter the counseling, is seen as a “surgeon’s mistake” by the patient. This requires very accurate flap development and template design and in patients with short foreheads and large volume requirements, preoperative tissue expansion may well be required. 10 Once the flap is accurately designed and double-checked prior to flap elevation, the nose, including the defect, is thoroughly injected with lidocaine and epinephrine and the wound edges from the Mohs surgery are sharply excised back to clean healthy bleeding edges. 11 At this point, the entire forehead, except for the portion of elevated flap, is also injected with dilute lidocaine with epinephrine. The flap outline is very carefully scored with a beaver blade and then a small distal incision is drawn on the flap and this is considered to be the handle, as well as the dog-ear excision and the handle is utilized for the entire flap elevation to minimize or eliminate handling of the reconstructive portion of the flap itself. Initially, the flap is elevated in the deep subcutaneous plane at the thickness of the requested inset at the point that the forehead flap can be determined to be closed, primarily if the flap elevation extends to the subfrontalis and then approximately 1.5 cm above the brow, the flap dissection is extended subperiosteally. Understand that this captures the perforators as described by Reece et al and contributes to flap vascularity. 12 The flap axis of rotation is below the brow and, if required, the flap incision itself can be extended and elevated to below the eyebrow with sharp dissection. If further length is required and is restrained by the periosteum, the periosteum itself can be scored under loop magnification, taking care to avoid injuring the axial vessels. It is important to Bovie electrocautery both the corners of the flap incisions because these will have zero tension on them at the conclusion of the case and can often contribute significantly to postoperative bleeding. Once elevated and rotated into position taking care to avoid excessive flap redundancy, a fresh no. 10 blade is used to thin the flap to the appropriate flap inset thickness. Understand that the distal quarter of the flap will likely never be re-elevated again and this portion needs to be thinned to match the final inset. The thickness of the flap is determined by the final requirements and whether a two- or three-staged flap is planned, as well as some assessment of a patient’s vascularity and as a rule for forehead flaps performed on smokers, no attempt is made to thin the flap except for the distal quarter. With a properly designed forehead flap, the elevation and actual inset should be the easiest part of the procedure. Final inset sutures are placed at the given alar margins of the flap and then it is very efficiently inset with 5–0 black nylon suture. Before flap inset, great consideration must be given to accurate closure of the forehead. The forehead itself is often forgotten and hastily closed, without considering the final cosmetic result. Understand that with a properly executed and inset forehead flap, the final nasal deformity can often be near invisible and the sole remaining deformity will be an unsightly forehead scar. For this reason, great attention should be directed to meticulous closure of the forehead. Care is taken to not close the forehead and pinch the pedicle. 1.5cm of unclosed skin should be maintained above the pedicle base. The remainder of the forehead is closed with 3–0 Vicryl sutures and then closely spaced 5–0 nylon sutures for skin closure. Oftentimes, a forehead will not be able to be closed given the initial size of the flap and for this reason, the forehead is either left open or extracellular matrix is applied to expedite healing. It is important to dismiss the idea of being able to close all of the forehead defects and the surgeon should not limit the size of the nasal flap based on amount of forehead skin available for a complete closure. The forehead does not require final closure and will heal with superb results if allowed to heal secondarily.
After the flap is inset, a significant amount of attention needs to be directed to postoperative dressings. Any active bleeders along the flap pedicle undergo either Bovie cautery or surgical clip application and all active bleeders are addressed prior to flap dressing. The most caudal portion of the Mohs surgical defect undergoes Bovie cautery, given this portion is not fully covered by the forehead flap and will often bleed, contributing to postoperative bleeding and possibly preventing the adherence of the flap to the defect. When all visible signs of bleeding have undergone cautery, the flap itself is wrapped, an H pattern of oxidized cellulose is designed to fit on the back of the flap without barber poling the flap itself because bleeding onto the oxidized cellulose can cause a postoperative blood cast and contribute to flap ischemia. 7 Understand that forehead flaps are often blue on elevation and rotation and although these looks can be alarming, great faith has to be placed in the robustness of the flap given that they ever rarely fail. Nitropaste is routinely applied to the distal portion of the forehead flap and then antibiotic surgical ointment is placed across the flap incision, as well as the flap pedicle itself and then the surgical dressing is wrapped around it to cover every exposed suture line. 13 The patient is followed up in the operating room for a period of 5 to 10 minutes to ensure that no bleeding persists because it is much easier to control bleeding in an operative setting than in the recovery room (▶ Fig. 13.2).
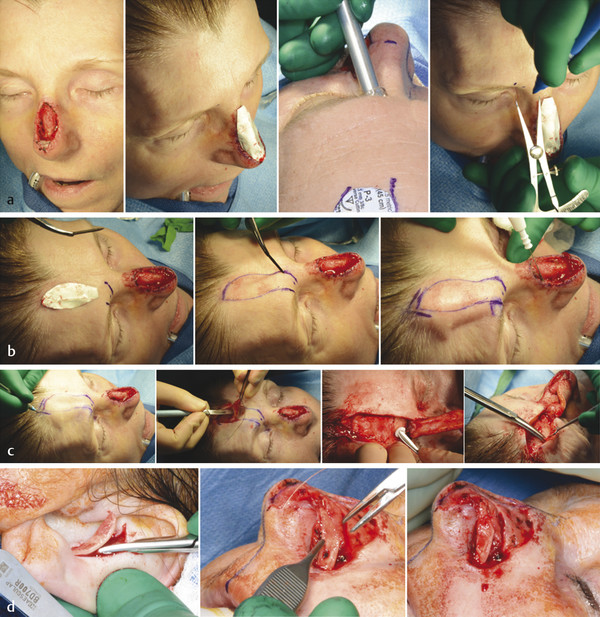
Fig. 13.2 (a) Foil pattern template is made with care taken to include convexity of nose. Supratrochlear artery is identified with Doppler at a single point below the medial eyebrow. Calipers are used to center pedicle design over identified arterial pedicle. (b) Flap is outlined, and marks are made to realign forehead on closure. Superior aspect of defect undergoes Bovie cautery to eliminate potential source of bleeding. (c) Perimeter of flap is scored and flap elevation begins with standing cone (to be excised later). Flap is elevated in deep subcutaneous plane, transitioning to subperiosteal 1–2 cm above the eyebrow. Periosteum is bluntly dissected to below the eyebrow if needed. Minimal undermining is performed only lateral to the pedicle. (d) If needed, conchal cartilage is elevated from an anterior incision. Nonanatomic cartilage graft is secured with 4–0 Vicryl suture. (f) Significant attention is directed for postoperative dressings. Any actively bleeding flap vessels undergo electrocautery, the flap is covered in nitropaste, and the incision lines are coated with antibiotic ointment.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


