Muscle-Sparing Free Transverse Rectus Abdominis Myocutaneous (TRAM) Flap
Arash Momeni
Liza C. Wu
DEFINITION
Acquired amastia following mastectomy is associated with significant psychological distress.1
Breast reconstruction following prophylactic mastectomy or mastectomy for breast cancer has been demonstrated to improve health-related quality of life and patient-reported outcomes.2
Favorable long-term patient satisfaction is particularly associated with autologous breast reconstruction using abdominal tissue.3,4,5
In contrast to the traditional free TRAM flap in which the entire width of the rectus abdominis muscle is harvested, the muscle-sparing free TRAM flap only incorporates a small amount of rectus abdominis muscle along with overlying anterior rectus sheath, thus, reducing donor-site morbidity.
ANATOMY
The rectus abdominis muscles are flat muscles located on either side of the midline that originate from the 6th to 8th costal cartilages and the xiphoid process and insert on the pubic symphysis.
Each rectus abdominis muscle rests within a fascial sheath (ie, rectus sheath) that is formed by the confluence of the aponeuroses of the oblique (external and internal) and transversus abdominis muscles.
Above the arcuate line, the aponeurosis of the internal oblique splits, thus contributing to the anterior and posterior rectus sheath by joining with the external oblique aponeurosis and transversus abdominis aponeurosis, respectively.
Below the arcuate line, all three aponeuroses form the anterior rectus sheath.
The rectus abdominis muscle has a dual blood supply via the superior and deep inferior epigastric vascular arcade.
These vessels originate from the external iliac vessels.
Perforating vessels from these arcades pierce the rectus abdominis muscle to perfuse the overlying skin and soft tissues.
The blood supply to the lower anterior abdominal skin via the superior epigastric artery is indirect and relies on “choke” vessels located in the midabdomen.
In contrast, perforators emanating from the deep inferior epigastric artery represent a more direct source of blood supply to the lower anterior abdominal skin.
This represents the anatomic basis for the more robust blood supply of the free muscle-sparing (MS) TRAM flap compared to the pedicled TRAM flap.
PATIENT HISTORY AND PHYSICAL FINDINGS
The preoperative evaluation for patients presenting for autologous breast reconstruction using an MS-TRAM flap includes a detailed history and focused physical examination.
History
Preoperative smoking cessation is strongly encouraged in order to decrease the risk of wound infection, mastectomy skin necrosis, and abdominal flap necrosis.6
Pre-existing medical conditions, such as diabetes mellitus, hypertension, etc., need to be optimized preoperatively.
Obesity is a specific consideration that may lend itself to increased intraoperative and postoperative complications such as increased blood loss, wound healing issues, and hernia formation.7
Physical examination
The abdomen is inspected for pre-existing scars that may preclude MS-TRAM flap harvest.
Although appendectomy and Pfannenstiel scars do not pose clinical problems (unless the deep inferior epigastric vessels were previously ligated), subcostal incisions can be associated with a higher rate of delayed wound healing due to compromised perfusion to the watershed area of the abdominal flap.
Midline scars are not necessarily problematic, particularly in bilateral reconstructions.
Merely unilateral reconstructions in patients with large breasts in whom more than two perfusion zones are required may occasionally necessitate raising the MS-TRAM flap as a bipedicled flap.
Previous liposuction is not a contraindication; however, a true abdominoplasty is.8
Palpation of the abdomen is performed to document the presence of ventral and/or umbilical hernias.
Repair of an umbilical hernia at the time of autologous breast reconstruction risks the development of umbilical necrosis.
The height of the MS-TRAM flap is determined preoperatively and should correspond to breast width.
It may be helpful to determine the degree of abdominal tissue laxity by having the patient flex at the waist, as this gives a reasonable estimate of how much tissue can be harvested without subjecting the closure line to undue tension.
Breast examination/palpation is important to assess preoperative beast volume as this can necessitate modification of flap design to optimize a volume match.
IMAGING
Preoperative imaging is not routinely required prior to MS-TRAM flap harvest.
Only in select patients, ie, patients with previous abdominal procedures in which the deep inferior epigastric vessels or its perforators were at risk for injury, is a CT angiography obtained to confirm the presence of suitable vessels.
SURGICAL MANAGEMENT
Parameters to consider include the following:
Timing of reconstruction
Immediate vs delayed reconstruction
Immediate reconstruction has several advantages. These include the ability to reconstruct a breast mound in a single procedure as well as ease of obtaining an aesthetically appealing result due to the presence of the breast skin envelope.
Delayed reconstruction can be offered at anytime after mastectomy and adjuvant chemotherapy. In cases of postmastectomy radiotherapy, we recommend waiting 6 months after the end of radiation to allow for the recovery of the soft tissues from radiation injury. Furthermore, scarred or irradiated skin that prevents adequate ptosis should be excised and replaced with abdominal skin.
Need for adjuvant radiotherapy
Radiotherapy after MS-TRAM flap-based reconstruction can result in volume loss, skin contracture, fat necrosis, and poor appearance.9
Options to remedy the detrimental radiation-induced effects include a “delayed-immediate” approach, in which a tissue expander is placed immediately and eventually replaced with autologous tissue following completion of radiotherapy, or immediate reconstruction with an MS-TRAM flap that is designed approximately 10% to 15% larger than the contralateral breast to account for the anticipated volume loss.
Recipient vessels
The decision as to whether the ipsilateral or contralateral MS-TRAM flap is used is predominantly determined by the choice of the recipient vessels (see Techniques).
Preoperative Planning
Preoperative patient assessment should reveal the presence of adequate amount of lower abdominal soft tissue for the purpose of breast reconstruction.
Clinical examination should rule out pre-existing abdominal scars that would preclude the harvest of an MS-TRAM flap.
Preoperative landmarks include the umbilicus, anterior superior iliac spines (ASIS), and the suprapubic crease.
The elliptical skin island of the MS-TRAM flap includes the areas between the upper border of the umbilicus and the suprapubic crease and the ASIS bilaterally.
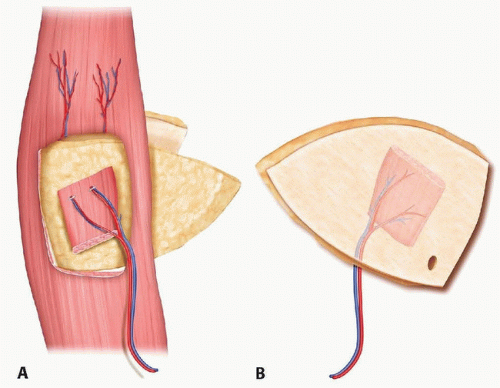 FIG 1 • A,B. Illustration of a free MS-TRAM flap based on the deep inferior epigastric vessels with limited rectus abdominis muscle attached to the skin island. (Courtesy of D.W. Low, MD.) |
Positioning
The patient is positioned supine on the operating table with bilateral upper extremities abducted.
The operating table should allow hip flexion to decrease tension during donor-site closure.
Approach
The lower abdominal skin can be harvested in a variety of different ways based on the amount of rectus muscle included as well as its vascular pedicle.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree