Fig. 35.1
Blisters surrounded by erythema on the gingiva and area of normal mucous membrane
Fig. 35.2
Erythema and large flaccid bullous lesions on the soft palate
Fig. 35.3
The tweezers sign is demonstrated on the gums

Fig. 35.4
Glazed appearance of the gingiva due to atrophy

Fig. 35.5
Blister and erythema on the mandibular gingiva and lichen planus-like lesions on the neck of a tooth
Ocular lesions occur in around 50 % of patients. They usually begin with unilateral chronic conjunctivitis that progresses to involve both eyes (Fig. 35.6). They are followed by subepithelial fibrosis, resulting in shrinkage of the inferior fornix. Fibrous tracts fuse the bulbar and palpebral conjunctivae, resulting in symblepharon formation (Fig. 35.7). Entropion and trichiasis can also occur and be responsible for superficial keratopathy, corneal ulceration, and vascularization, ultimately resulting in blindness (Fig. 35.8) [15].
Fig. 35.6
Erythema of the palpebral and bulbar right conjunctivae and shortening of the right fornix
Fig. 35.7
Inferior forniceal shortening and symblepharon formation of the left eye
Fig. 35.8
End-stage ocular MMP. Surface keratinization, absence of inferior fornix, and corneal vascularization of the right eye
ENT involvement is present in at least 35 % of patients as demonstrated in a prospective study of 110 MMP patients [11]. Nasal symptoms consist of nasal crusting, nasal airway obstruction, or recurrent epistaxis; they are related to atrophic and crusted rhinitis and nasal erosions. Pharyngeal symptoms include sore throat, dysphagia, or odynophagia. Examination of the pharyngeal area may reveal erythema and erosions of oropharynx or velopharyngeal stenosis.
Laryngeal symptoms correspond to dysphonia, such as hoarseness or stridor, and dyspnea. The most frequent laryngeal lesions are erosions of the epiglottal laryngeal surface (Fig. 35.9). Erosions and edema are also seen on the arytenoids and aryepiglottic or interarytenoid folds. Synechiae between the nasal septum and inferior turbinate, choanal stenosis, pharyngeal synechiae, laryngeal synechiae, and laryngeal stenosis may be encountered. Tracheal and bronchial erosive lesions have been reported rarely and may evolve into stenosis resulting in dyspnea, respiratory failure, and death [16].
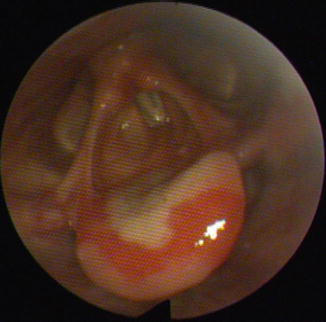
Fig. 35.9
Large fibrinous erosion surrounded by erythema on the laryngeal surface of the epiglottis
Esophageal manifestations are rare (less than 5 %) and may be suspected in cases of dysphagia, odynophagia, aspiration, and chronic cough. Endoscopy demonstrates erosions (Fig. 35.10a) and webs (Fig. 35.10b), and strictures of the upper third of the esophagus are often present [17]. Stenosis can also be evidenced by barium swallow using early phase of swallowing radiographs focused on the neck.

Fig. 35.10
Esophageal webs (a) and several erosions of the esophagus (b) observed by endoscopy
The genitalia may be involved in 15 % of MMP patients. Lesions may be asymptomatic. Complaints include discomfort, dysuria, and vulvar pain in females. In females, erosive vestibulitis and erythematous erosions on the labia minora and majora are seen, evolving into lichen planus-like scars (Fig. 35.11), and/or synechiae, with fusion of the labia minora and narrowing of the introitus (Fig. 35.12) [18, 19]. In males, erosions may develop over the glans penis and particularly on the coronal sulcus; scarring results in tethering of the foreskin to the glans penis (Fig. 35.13) and rarely phimosis or urethral stenosis [20].



Fig. 35.11
Vulvar erosions and lichen planus-like scars in a MMP patient previously followed for a presumptive diagnosis of erosive lichen planus for several years
Fig. 35.12
Vulvar lichen planus-like lesions and fusion of the labia minora
Fig. 35.13
Asymptomatic fibrinous ulceration on the foreskin and fusion of the coronal sulcus
Lesions on the mucosal surfaces of the anus are seen in less than 10 % of MMP patients. Lesions may be asymptomatic and patients often neglect anal signs or think they are simple hemorrhoids (Fig. 35.14). Perianal erythema, erosions, lichen planus-like lesions, and scarring are usual and severe involvement may result in complete stenosis and epithelialization of the anal orifice [21].

Fig. 35.14
Large asymptomatic geometrical erosion on the anus and perianal area
Skin involvement is encountered in about 25 % of MMP patients. The blisters are often rare and scattered over erythematous plaques of the head, the neck, or the trunk, but generalized blistering has been reported [22]. Lesions heal with milia and atrophic scars (Fig. 35.15) which can lead to scarring alopecia on the scalp. There is no pruritus.

Fig. 35.15
Multiple pigmented and atrophic scars with milia observed on the back after healing of blisters in a MMP patient misdiagnosed as bullous pemphigoid for 3 years
35.2.2 Brunsting-Perry Pemphigoid
Brunsting-Perry pemphigoid is a variant of MMP. Patients present with vesicles and blisters located only over the head, the neck, and the upper aspect of the trunk. In contrast to the classical form of MMP, they have no mucous membranes involvement. Cutaneous lesions heal with atrophic scarring.
35.2.3 Single-Site Forms
Certain patients with MMP exhibit lesions restricted to a single mucous membrane, most common among these being oral MMP followed by pure ocular MMP [15]. Other single-site forms involving only the esophagus [23] or vulva [18] have been reported. However, it is important to keep in mind that involvement of other mucous membranes may present a long time after the initial onset of the disease: esophageal involvement has been reported 10 years after the beginning of MMP [17]. This entails following the patients with MMP for a prolonged period to avoid serious complications involving the eye, larynx, or esophagus. Asymptomatic involvement of other mucous membranes may also be underestimated by medical specialists who do not perform systematic and complete physical examination of the patients.
35.2.4 Anti-laminin-5 Cicatricial Pemphigoid
Patients with this particular form of MMP are clinically indistinguishable from patients with the classical form of MMP. Only immunological criteria allow the ascertainment of this diagnosis. The oral and ocular mucous membranes and also the skin are most commonly involved [24]. The severity of the bullous disease seems more important than in the classical form because of a high level of esophageal [25] and laryngeal [26] involvement and an increased MMP severity score [25]. This form appears to be associated with an increased risk for solid cancer, especially in the first year after blister onset [24], but this association has not been found in our experience [25].
35.3 Staging
It is important to evaluate the extent of MMP since it will determine the management, prognosis, and treatment. Two staging classifications for ocular involvement have been developed in parallel by Mondino and Brown [27] and by Foster et al. [28]. The Mondino scoring system relied on the shortening of the conjunctival fornix. Stage I has less than 25 % shortening, stage II 25–50 %, stage III has about 75 %, and stage IV is defined as end-stage ocular MMP. The Foster classification is based on the progression of conjunctival fibrosis: stage 1 for chronic conjunctivitis, stage 2 for shortening of the fornix, stage 3 for the appearance of symblephara, and stage 4 as end-stage disease with ankyloblepharon and extreme ocular surface keratinization. Grading of conjunctival inflammation is performed in parallel. Afterwards these two ocular staging systems have been combined to improve their sensitivity [29]. Then a scoring system taking into account all the potentially affected mucous membrane has been developed by dermatologists [30]. It has been improved by Le Roux-Villet et al. in order to take into account anal and tracheal mucous membrane and to do discrimination between active and cicatricial lesions [31].
35.4 Positive Diagnosis
Routine skin biopsy tests such as standard histopathology and direct immunofluorescence (IF) allow the diagnosis of autoimmune subepithelial blistering disease but do not specify a diagnosis of MMP with certainty. Specialized tests available in only certain laboratories are necessary to confirm MMP.
35.4.1 Standard Pathology
Routine skin biopsy shows a subepidermal blister with an intact epidermis and a dermal inflammatory infiltrate of lymphocytes, mononuclear cells, neutrophils, and some eosinophils. In affected mucosal tissues, subepithelial clefts (Fig. 35.16) or erosions are present and are subtended by a mixed inflammatory infiltrate; fibrosis is seen in more advanced lesions. If standard microscopy was performed, alteration of the lamina densa (Fig. 35.17) should be observed explaining wound healing delay and atrophic scars.

Fig. 35.16
Standard pathology of buccal mucosa showing a subepithelial cleavage
Fig. 35.17
Standard electron microscopy of MMP cutaneous lesion demonstrating focal destruction of the lamina densa of the basement membrane zone
35.4.2 Direct Immunofluorescence
Patients with MMP have linear deposits of immunoglobulins and complement along the BMZ of the skin, buccal mucosa, conjunctiva, genitals, or even esophagus. Immunoglobulin G is the immune reactant most frequently detected by direct IF, but IgA in 50 % of cases and IgM can also be present (Fig. 35.18). Direct IF is mostly positive but could be negative in pure ocular MMP. In this case immunoperoxidase is more sensitive than direct IF in detecting immunoreactants along the conjunctival BMZ [32].
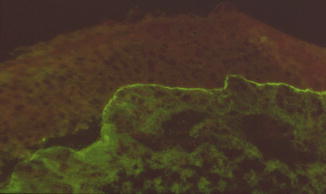
Fig. 35.18
Direct immunofluorescence of nasal mucosa showing linear deposits of IgG along the basement membrane zone and demonstrating the specificity of atrophic rhinitis
35.4.3 Direct Immunoelectron Microscopy
Direct immunoelectron microscopy permits localization of which precise structure of basement membrane zone the autoantibodies of the patients are binding in vivo. It is the “gold standard” for the diagnosis of MMP, allowing to assert the diagnosis with a very good sensitivity. Immunoreactivity in MMP patients is typically observed on the lamina densa related to intense deposits of antibodies directed to BP180. Immunoreactants may extend to the lamina lucida, but usually a clear space between immune deposits and the membrane of keratinocytes is visible. Immune deposits are present on the roof and the floor if skin is splitted. In patients with anti-laminin-5 antibodies, immune deposits are present on the lower part of the lamina lucida and on the floor of the splitted skin if a cleavage occurs. They are located under the lamina densa on the anchoring fibrils in patients with the cicatricial pemphigoid-like form of EBA.
Related posts:
 Kindlin-1 and Its Role in Kindler Syndrome
Kindlin-1 and Its Role in Kindler Syndrome
 Cyclophosphamide in Autoimmune Blistering Diseases: Safety, Efficacy and Evidence Base
Management of Bullous Systemic Lupus Erythematosus
Cyclophosphamide in Autoimmune Blistering Diseases: Safety, Efficacy and Evidence Base
Management of Bullous Systemic Lupus Erythematosus
 Using Intravenous Immunoglobulins in Autoimmune Bullous Diseases
Using Intravenous Immunoglobulins in Autoimmune Bullous Diseases
 Living with Epidermolysis Bullosa: Reviewing the Impact on Individuals’ Quality of Life
Living with Epidermolysis Bullosa: Reviewing the Impact on Individuals’ Quality of Life
 Dermatitis Herpetiformis
Dermatitis Herpetiformis
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


